Download
1 / 25
260 likes | 429 Views
ACE inhibitors and the Kidney. William G. Paxton, MD, PhD Nephrology Medical Associates of GA. At what creatinine do you stop using an ACE inhibitor?. Let’s think about the physiology!. History of RAS. 1898 Tigerstedt “Renin” 1930’s Angiotonin/Hypertensin - “Angiotensin”

E N D
ACE inhibitors and the Kidney William G. Paxton, MD, PhD Nephrology Medical Associates of GA
History of RAS • 1898 Tigerstedt “Renin” • 1930’s Angiotonin/Hypertensin - “Angiotensin” • 1977 Captopril developed • 1991 AT1 Receptor Cloned • 1996 Losartan
Angiotensinogen Renin Angiotensin I Bradykinin ACE ACEi Non ACE (-) (-) Angiotensin II Inactive Metabolites ARB AT2 Receptor AT1 Receptor
Vasoconstriction • Aldosterone synthesis and release • Induces salt and water reabsorption • Mediates thirst, salt appetite • Secretion of vasopressin • Growth factor Angiotensin II (Ang II) Octapeptide hormone Asp - Arg - Val - Tyr - Ile - His - Pro - Phe Physiological effects
Angiotensin II Binds to cell surface receptors Two receptor subtypes AT Expressed in mature tissues 1 Blocked by losartan (DuP 753) AT Expressed in fetal tissue 2 Blocked by PD 123177 AT receptor mediates all known physiological effects * 1
The Kidney (AT1 Receptors) • Afferent and Efferent Arterioles • Mesangial Cells • Renal Medulla (esp. inner stripe of outer medulla) • Juxtaglomerular Cells
ACEi in Hypertension • Relaxes vascular smooth muscle • Inhibits salt and water reabsorption (aldo) • Inhibits water seeking behavior
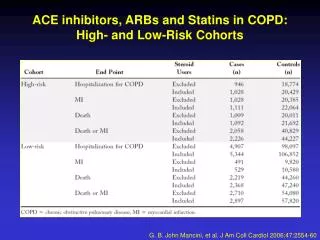
Clinical Indications for ACEi • Hypertension • CHF • S/p MI • Diabetes Mellitus • Proteinuria • Vascular Disease • Post - transplant
The Kidney • Decreases Proteinuria (DM and Non-DM) • Beneficial effect on permeability • Beneficial effect on size selectivity • Slow the Rate of GFR Decline
The Heart - Organ • Prevents cardiac hypertrophy • Limits infarct size • Improves cardiac function • Improves cardiac metabolism
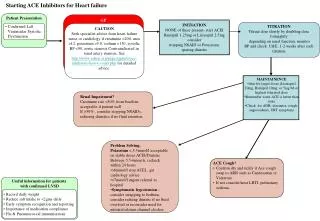
HOPE • 9297 Patients • Age >55 • Vascular Disease/DM + 1 other CV factor • Normal EF (>40%) • Ramipril (10mg) vs. Placebo
HOPE • MI • Stroke • Death (CV causes)
HOPE (Primary endpoints) • Death (CV) - 6.1 vs 8.1 P<0.001 RR=0.75 • MI - 9.9 vs 12.2 P<0.001 RR=0.80 • Stroke - 3.4 vs 4.9 P<0.001 RR=0.69
HOPE (secondary endpts.) • Death 10.4 vs 12.2 • Revascularization 16.0 vs 18.6 • Cardiac arrest 0.8 vs 1.2 • Heart Failure 7.4 vs 9.4 • DM complications 6.2 vs 7.4 * all statistically significant
Summary • RAS has many effect on different tissues • ACEi and ARBs not equvalent • Many clinical indications for ACEi