Download
1 / 56
560 likes | 578 Views
Explore the intricate details of the spinal cord, from its structure to functions and various disorders, such as tumors, infections, and vascular diseases. Learn about classical syndromes and conditions like multiple sclerosis and Brown Sequard Syndrome.

E N D
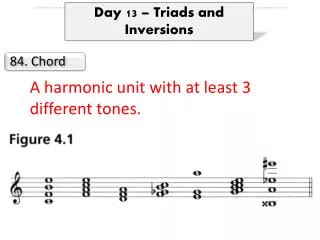
Spinal cord & Spinal Nerves • The spinal cord (45cm long) is part of the central nervous system and is connected to the brain • Extends from the foramen magnum to the first lumbar vertebra (L1). • The spinal cord is the main pathway for information connecting the brain and peripheral nervous system. • 31 pairs of spinal nerves
Spinal Cord Protection Bony Canal- vertebral canal Connective tissue- meninges Cushion of cerebrospinal fluid (CSF)- CSF acts as a shock absorber
Meninges • The meninges surround, protect, & stabilize the CNS • Consist of 3 layers • DURAMATER • ARACHNOID • PIAMATER
Meninges • Epidural space- a space between bony canal & dura mater • Subdural space- A space between the dura mater & arachnoid mater- contains interstitial fluiid • Subarachnoid space- contains CSF fluid
Internal Anatomy of Spinal cord • Gray & white mater • H- shaped gray matter (central zone): dorsal & ventral horns • White matter (outer zone): - arrange in columns
Spinal Cord levels The greatest amount of grey matter (cells) is largest in the spinal segments of the cervical and lumbosacral enlargements
White mater (regions) • Anterior white column • Posterior white column • Lateral white column
Functions of spinal cord Spinal cord reflexes: A reflex is a fast , involuntary, unplanned sequence of actions occur in response to a particular stimulus Integration of information highway for upward and downwardtravel of sensory and motor information
Traumatic Spinal Cord Disease • 10,000 new spinal cord injuries per year • MVA, sports injuries the most common • Victims under 30 yrs old, male>>females • Fx/dislocation of vertabrae most likely to occur at: • C5,6 • T12, L1 • C1,2
Tumors • Metastatic or primary • Extramedullary • Extradural - most common • Bony - breast, prostate • Intradural - very rare • Meninges - meningioma • Nerve root - schwannoma • Intramedullary - very rare • Metastatic • Primary - astrocytoma or ependymoma
Intramedular tumors • Anterolateral column compression lead to sensory (thermoalgesic) loss that extends lower as the tumor grows
Lateral compression • Sensory disturbance appears first in the sacrate dermatoma; as the tumor grows, the sensory problems ascend upwards to the level of the lesion
Transverse myelitis • Inflammation of the spinal cord • Post-infectious • Post-vaccinial • Multiple sclerosis • Pain at level of lesion may preceed onset of weakness/sensory change/b&b disturbance • Spinal tap may help with diagnosis
Infections Involving the Spinal Cord • Polio • only the anterior horn cells are infected • Tabes dorsalis • dorsal root ganglia and dorsal columns are involved • tertiary syphillis • sensory ataxia, “lightening pains” • HIV myelopathy • mimics B12 deficiency • HTLV-1 myelopathy - • tropical spastic paraparesis
Multiple Sclerosis • Demyelination is the underlying pathology • Cord disease can be presenting feature of MS or occur at any time during the course of the disease • Lesion can be at any level of the cord • Patchy • Transverse • Devic’s syndrome or myelitis optica • Transverse myelitis with optic neuritis
Vascular Diseases of the Spinal Cord • Infarcts • Anterior spinal artery infarct • from atherosclerosis, during surgery in which the aorta is clamped, dissecting aortic aneurysm • less often, chronic meningitis or following trauma • posterior columns preserved (JPS, vib) • weakness (CST) and pain/temperature loss (spinothalamic tracts) • Artery of Adamkiewicz at T10-11 • Watershed area • upper thoracic
Vascular Diseases of the Spinal Cord, cont • Arteriovenous malformation (AVM) and venous angiomas • Both occur in primarily the thoracic cord • May present either acutely, subacutely or chronically (act as a compressive lesion) • Can cause recurrent symptoms • If they bleed • Associated with pain and bloody CSF • Notoriously difficult to diagnose • Hematoma - trauma, occasionally tumor
Other Diseases of the Spinal Cord • Hereditary spastic paraparesis • Usually autosomal dominant • Infectious process of the vertabrae • TB, bacterial • Herniated disc with cord compression • Most herniated discs are lateral and only compress a nerve root • Degenerative disease of the vertabrae • Cervical spondylosis with a myelopathy • Spinal stenosis
Brown Sequard Syndrome • Cord hemisection • Trauma or tumor • Dissociated sensory loss • loss of pain and temperature contralateral to lesion, one or 2 levels below • crossing of spinothalamic tracts 1-2 segments above where they enter • loss of vibration/proprioception ipsilateral to the lesion • these pathways cross at the level of the brainstem • Weakness and UMN findings ipsilateral to lesion
Syringomyelia • Fluid filled cavitation in the center of the cord • Cervical cord most common site • Loss of pain and temperature related to the crossing fibers occurs early • cape like sensory loss • Weakness of muscles in arms with atrophy and hyporeflexia (AHC) • Later - CST involvement with brisk reflexes in the legs, spasticity, and weakness • May occur as a late sequelae to trauma • Can see in association with Arnold Chiari malformation
Conus Medullaris vs. Cauda Equina Lesion FindingConusCE Motor Symmetric Asymmetric Sensory loss Saddle Saddle Pain Uncommon Common Reflexes Increased/Decreased decreased Bowel/bladder Common possible
B12 Deficiency • Subacute combined degeneration of the cord • B12 deficiency • malabsorption of B12 secondary to pernicious anemia or surgery • insufficient dietary intake - vegan • Posterior columns and CST involvement with a superimposed peripheral neuropathy
Degeneration of the long spinal pathways (both ascending and descending) and the peripheral nerve fibers
Clinical presentation • Gait abnormalities • Ataxia • Speech disorders • Nistagmus • Hyporeflexia • Trophic changes • High plantar arches (pes cavus deformity of the foot) • Sensory disturbance • Babinski sign
Clinical presentation • Symptoms typically begin sometime between the ages of 5 to 15 years, • scoliosis • Diabetes (about 20% of people with Friedreich's ataxia develop carbohydrate intolerance and 10% develop diabetes mellitus) • Heart disorders (e.g., atrial fibrillation, and resultant tachycardia (fast heart rate) and hypertrophic cardiomyopathy ) • These symptoms are slow and progressive. Long-term observation shows that many patients reach a plateau in symptoms in the patient's early adulthood.
Genetics • Autosomal recesive disorder • Mutation of frataxin gene (9q13-q21) • Long arm of cromosome 9 • Prevalence 1 : 50.000 • Genetic counselling!
Treatment • Physical therapy • Nerve and muscle trophic drugs • Treatment of complications • Treatment of heart disorders
Lateral Amiotrophic Sclerosis (ALS) • Degenerative disease of the central nervous system • Degeneration and death of motor neurons, both in the cortex and in the spine • Mean survival time is 3 to 4 years from diagnosis USA – “Lou Gehrig’s disease”
ALS – clinical picture • progressing motor deficit • Signs related both to upper and to lower motor neuron damage • starting age is around 60 years (20-80 years) • Involvement of any part of the CNS • Either as UMN damage or as LMN damage
SLA – clinical picture • Muscle weakness • In 60-85% of pts starts in the limbs and in 15-40% starts with bulbar signs • Atrophy • Stiffness • Cramps • Fasciculations; • Highly suggestive for ALS if largelly distributed and accompanied by UMN damage siogns
SLA – clinical picture • Respiratory Insufficiencyis seldom present from the start • Dispnea, asteny, weak cough, predisposition for developping pneumonia ant athelectasies • With time, LMN signs may overcome all of the UMN signs • Brainstem damage signs • disphagia • disarthrie • sialorrhea (reduction of swallowing) • laringospasm • Lately in the course of disease oculomotor problems
ALS • EMG criteria for ALS (Lambert): • Normal sensory conduction velocity • Motor conduction velocities normal or nearly normal, depending of the muscke waisting • Fibrilation and fasciculations • Increased amplitude and duration of action potentials • EMG is only accesory to diagnosis in ALS
Evaluation and follow up • Global evaluation scales for ALS: • Scoring based on subjective and clinical data • Muscle force measuring • Evaluation of quality of life
Treatment • Maintaining a good quality of life as long as possible • Prolongation of active life • Prolongation of life expectancy
Negative results Vitamin E TCH346 Celebrex Creatine Indinavir Topiramate(topamax) Neurontin Minocycline Other drugs Lithium Arimoclomol Ceftriaxone Manganoporphirin Drug Trials
Medical ManagementRiluzole • The only FDA approved drug for ALS treatment • Approved for use in the US, Europe- 1996 and Canada –2000 • Safe, fairly well tolerated • Moderate efficacy • Expensive ($10,000/year !!) • Prolongs survival by 3-4 months, Cochran review 2005 • Side effects include fatigue, nausea, diarrhoea and liver toxicity
Muscle weakness • Aerobics, exercises to improve flexibility, force • As the disease progresses the rehabilitation programme has to be adapted to possibilities • Establish safe exercises without overexertion • Maintaining independence • Assistive devices (wheel chair, cruches, walker, voice command, lifts, large doors, adapted vehicles)