Download
1 / 72
720 likes | 736 Views
Explore the causes, diagnostic methods, therapy options, and risk factors of osteoporosis, a condition affecting bone mass and fragility. Learn about fractures, bone density, and assessment techniques.

E N D
Osteoporosis – causes, diagnostics and therapyprof. Marek Bolanowski, MD, PhDDepartment of Endocrinology, Diabetes and IsotopeTherapy V ED Internal medicine, endocrinology
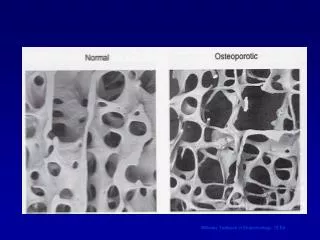
Osteoporosis • A systemic disease of the skeleton characterized by low bone mass and microarchitecture deterioration of bone tissue leading to bone fragility and susceptibility to fractures. • WHO 1994 • normal bone osteoporotic bone
Osteoporosis • A disease of the skeleton characterized by an increased risk of fractures resulting from reduced mechanical bone strength. • Reduced bone strength depends on bone mineral density (BMD) and the quality of bone tissue. NIH 2001
Causes of osteoporosis • genetic 75-85% • peak bone mass • hormonal • estrogen deficiency • environmental • feeding, movement
Osteoporosis • Primary (involution) • Postmenopausal type 1 • Senile type 2 • Secondary
Typical change of body profile 55 65 75
Bone mass and density • Peak bone mass childhood • Bone mass and density loss adulthood
Bone structure and turnover • Trabecular (cancellous) bone 20% of skeletal mass 80% of bone turnover • Cortical (compact) bone 80% of skeletal mass 20% of bone turnover
Osteoporotic fracture • A fracture that is disproportionate to the causative forces which occurs following a fall from the patient’s own height, after all other causes have been ruled out. • Low-trauma (pathological) fractures may occur for reasons other than osteoporosis (cancer, bone cyst, osteomalacia...)
Osteoporotic fractures • Spine • Ribs
Forearm Humerus Proximal femur Osteoporotic fractures
Most common fractures type of fracture forearm spine femur • age > 55 > 65 > 75 • F:M 4:1 3:1 2:1 • bone trabecular trabecular cortical
Fractures • familial predisposition, low bone mass and density, previous fractures, low body mass, high height, medication, tendency to falling • women – at home, men – outside home • 20% of women and 30% of men die within 1 yr after femur fracture • 40% remain immobilized forever
Risk factors for fractures • Falls • Low BMD
Risk factors for falls • Related to the patient’s condition • External (environmental)
Risk factors for falls related to the patient’s condition • A history of falls, fear of falling • Muscle weakness, arthralgia and arthritis • Gait/balance disorders • Visual impairment • Impairment of cogitive functions, depression, memory disorders • Urinary incontinence • Age > 65 yrs, low body mass • Use of more than 4 drugs, use of psychotropic and hypertensive drugs
Enivironmental risk factors for falls • Poor lighting conditions (at home) • Poor vision (no spectacles/glasses) • Obstacles on the patient’s way (at home) • Slippery, uneven surfaces (ice, snow, rain...) • Lack of position changes facilities (barriers in toilet or bathroom) • Transportation and public traffic
Reduced bone strength • BMD • Bone quality
Bone quality • Direct assessment • Histomorphometry • Microstructure in μCT/μMR • Mechanical forces (bending, twisting…) • Indirect assessment • Bone markers • QUS • BMD
Bone mineral density • BMD – objective measurement by DXA • BMD – best single predictor of fracture risk • BMD decrease = increase of fracture risk
Indications for densitometry • Estrogen deficiency • Changes on vertebral X-ray • Steroid therapy • Hyperparathyroidism or other diseases associated with osteoporosis • Male hypogonadism, alcohol abuse • Therapy monitoring
Sites of measurements • distal and ultradistal forearm • lumbar spine (antero-posterior or lateral projection) • proximal femur – femoral neck, trochanter major, Ward’s triangle, total femur • heel, patella, tibia • fingers (phalangi) • total body
SPA DPA SPX, SXA DXA, DEXA, DPX (dual energy X-ray absorptiometry) QCT QMR USG, QUS Methods of measurements
Densitometry • BMD • bone mineral density • (g/cm2) “areal thickness” • integration of density and thickness • (g/cm3) in computed tomography • BMC • bone mineral content • (g)
BMD - best predictor of fracture risk • positive correlation with skeletal strength • decreases with age • negative correlation with bone fractures occurence
Bone mineral density • BMD
decrease of BMD by 1 SD 2 - 4 fold increase of fractures occurrence
T-score • difference between measured BMD value and theoretical mean peak bone mass • expressed in standard deviation (SD) • age independent
Z-score • difference between measured BMD value and mean age-matched theoretical normal BMD • expressed in SD • both BMD dispersion in the normal population and age-related bone loss are regarded
A reflects T-score = -3.0 SD, and Z-score = -2.0 SD in 50 y.o. subject. B reflects T-score = -2.0 SD, ans Z-score = +1.5 SD in 80 y.o. subject.
Densitometric criteria of osteoporosis T-score • Normal between -1.0 and +1.0 SD • Osteopenia between -2.5 and -1.0 SD • Osteoporosis lower than -2.5 SD • Established lower than -2.5 SD osteoporosis + fracture(s)
calcifications deformities fractures fat in bones (medulla) position analysis wrong data infiltrations osteolytic metastases osteomalacia position analysis wrong data False results
Osteoporosis on X-ray • No more for diagnostics • When BMD loss more than 30% • Fractures • Deformities
Assessment of fracture risk • DXA and quantitative ultrasound • Clinical risk factors • Markers of bone turnover • Bone formation • Bone resorption
Clinical risk factors - CRF • Age • Sex • Body mass • Height • Previous fractures • Parental hip fracture • Current smoking • Steroids • Rheumatoid arthritis • Secondary osteoporosis • Alcohol > 3 units daily • Femoral neck BMD
Endocrine disorders Gastrointestinal disorders Malnutrition states Renal failure Cancer Transplantations Genetic disorders Locomotor system dysfunction Immobilization steroids immunosuppressants cytotoxic anticonvulsants heparin aluminium lithium GnRH agonists Conditions that increase risk of osteoporosisSecondary osteoporosis
Secondary osteoporosis • Bone loss, microarchitecture alterations and fragility fractures due to an underlying disease or medication. • Premenopausal women, younger men, not typical target population for routine osteoporosis screening. • Limited response to anti-osteoporosis therapy. • Secondary causes – 30% of osteoporosis in women. • Secondary causes – 70% of osteoporosis in men.
Conditions that increase risk of osteoporosis Endocrine disorders • Menstrual abnormalities/amenorrhoea • Hyperprolactinemia • Male hypogonadism • Primary hyperparathyroidism • Hyperthyroidism • Hypercortisolism – Cushing syndrome
Biochemistry calcium, phosphate urea, creatinine, GFR blood count, sedimentation glucose, HbA1c urine analysis monoclonal protein Hormonal PTH TSH, fT4, fT3 cortisol, ACTH PRL sex steroids 1,25-dihydroxycholecalciferol 25-OH-vit. D Laboratory tests