Download
1 / 1
10 likes | 145 Views
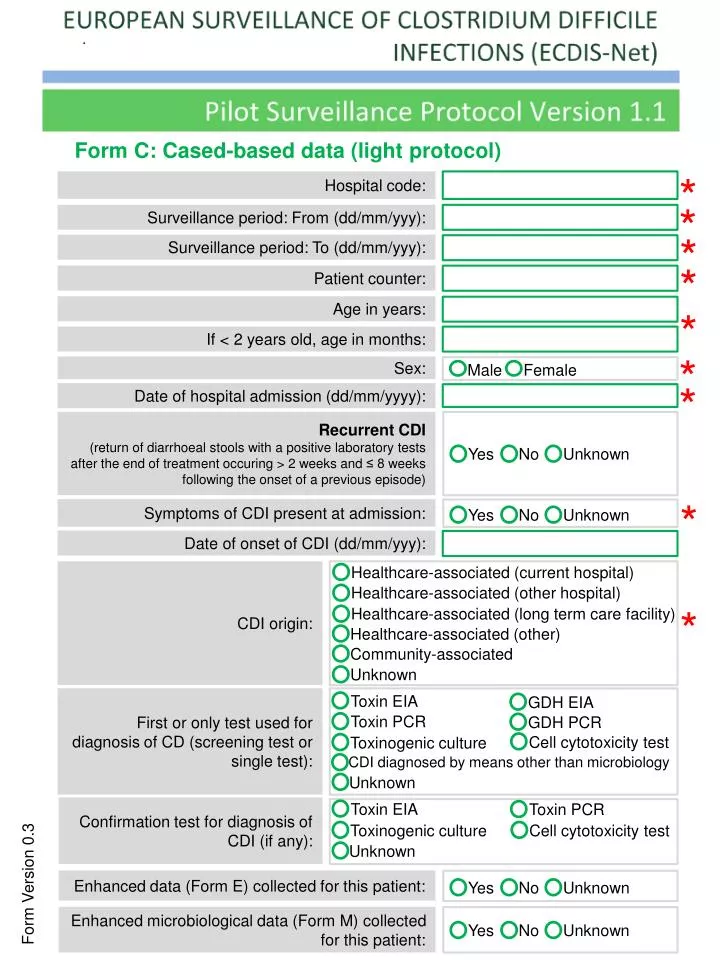
Form C: Cased-based data (light protocol ). *. Hospital code :. *. Surveillance p eriod : From ( dd /mm/ yyy ):. *. Surveillance p eriod : To ( dd /mm/ yyy ):. *. Patient counter :. Age in years :. *. If < 2 years old , age in months :. *. Sex:. Male. Female. Unknown.

E N D
Form C: Cased-based data (light protocol) * Hospital code: * Surveillanceperiod: From (dd/mm/yyy): * Surveillanceperiod: To (dd/mm/yyy): * Patient counter: Age in years: * If < 2 yearsold, age in months: * Sex: Male Female Unknown Unknown Yes No Unknown Unknown No No Yes No Yes Yes * Date ofhospitaladmission (dd/mm/yyyy): Recurrent CDI (returnofdiarrhoealstoolswith a positive laboratorytests after the end oftreatmentoccuring > 2 weeksand ≤ 8 weeksfollowingtheonsetof a previousepisode) * Symptoms of CDI present at admission: Date ofonsetof CDI (dd/mm/yyy): Healthcare-associated (currenthospital) CDI origin: Healthcare-associated (otherhospital) * Healthcare-associated (long term care facility) Healthcare-associated (other) Community-associated Unknown Toxin EIA GDH EIA First or only test used for diagnosis of CD (screening test or single test): Toxin PCR GDH PCR Cell cytotoxicity test Toxinogenic culture CDI diagnosedbymeansotherthanmicrobiology Unknown Toxin EIA Toxin PCR Confirmation test for diagnosis of CDI (if any): Cell cytotoxicity test Toxinogenic culture Unknown Form Version 0.3 Enhanced data (Form E) collected for this patient: Enhanced microbiological data (Form M) collected for this patient: