Download

1 / 1
10 likes | 214 Views
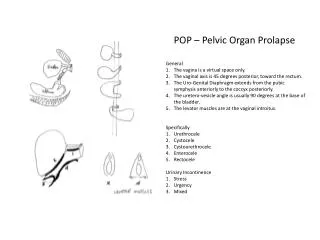
No. 050. Five-year functional outcomes in recurrent pelvic organ prolapse repair using mesh in the elderly. Chasta Bacsu , Vincent Tse Concord Repatriation General Hospital, Sydney, NSW, Australia. Introduction

E N D
No. 050 Five-year functional outcomes in recurrent pelvic organ prolapse repair using mesh in the elderly ChastaBacsu, Vincent Tse Concord Repatriation General Hospital, Sydney, NSW, Australia Introduction The safety and efficacy of mesh in pelvic organ prolapse (POP) repair is controversial.[1] There is established data on its use in abdominal sacrocolpopexy, and emerging data from randomised trials in cystocele repair. Most of these studies are of short to medium term. [2, 3] Literature relating to mesh use for POP repair reporting long-term outcomes in the elderly is especially scarce. Results Both questionnaires demonstrated improvement in all 3 domains. Aim To assess 5-year functional outcomes with quality of life (QoL) assessment in an elderly cohort with recurrent POP who underwent POP repair with mesh. To see if a staged protocol is appropriate in the elderly to avoid a concomitant sling procedure in patients with urodynamic stress incontinence undergoing POP repair. • Methods • Single-centre prospective cohort study of females over age 70 with recurrent POP who elected to have surgical repair using mesh from 2003 to 2009. • History, POP-Q staging and fluoroscopic urodynamics performed pre-operatively in all patients. • Informed consent included discussion of mesh or native tissue options. Only Amid type 1 mesh was used. • In our protocol, concomitant sling was not used in cases with urodynamic or occult SUI. • All patients assessed at 6, 12 months and at least once more during the study period until October 2011. • Primary outcome was quality of life following POP repair. • Assessed by: • Pelvic Floor Distress Inventory Short Form 20 (PFDI-SF20) • Pelvic Floor Impact Questionnaire Short Form 7 (PFIQ-SF7) Each questionnaire has a urinary, bowel and sexual function domain. • Linear mixed model with autoregressive covariance structure used in statistical analysis. p<0.001 PFIQ-SF7 Scores Time (months) p<0.001 PFDI-SF20 Scores Time (months) 1 had vaginal mesh extrusion that healed with topical estrogen. None required mesh excision. 3 of 18 with preoperative urodynamic SUI (17%) required mid-urethral sling post POP repair. SUI either improved or remained non-bothersome in 15 (83%) who did not desire a sling after their POP was treated. Conclusions Satisfactory long-term anatomical and functional outcomes can be achieved with minimal morbidity using mesh in the elderly for recurrent POP repair. Using a staged approach, only 17% of our patients with pre-op urodynamic SUI desired a sling post POP repair. Placement of mid-urethral slings at time of POP repair may result in overtreatment in this elderly group who may be more susceptible to complications and may have less physiological reserve to cope with such morbidities when they arise. References [1] Carey M, Higgs P, Goh J, Lim J, Leong A, Krause H, Cornish. Vaginal repair with mesh versus colporrhaphy for prolapse: a randomised controlled trial. BJOG 2009; 116: 1380-1386. [2] Altman D, Väyrynen T, Engh ME, Axelsen S, Falconer C. Anterior Colporrhaphy versus Transvaginal Mesh for Pelvic-Organ Prolapse. NEJM 2011; 364: 1826-1836. [3] Maher CM, Feiner B, Baessler K, Glazener CMA. Surgical management of pelvic organ prolapse in women: the updated summary version Cochrane review. IntUrogynecol J 2011; 22: 1145-1457. Acknowledgements Sister Karina So, Clinical Nurse Consultant Professor Jenny Peat with statistics Poster presentation sponsor






![get [PDF] Download Pelvic Organ Prolapse: The Silent Epidemic download](https://cdn7.slideserve.com/12583059/pelvic-organ-prolapse-the-silent-epidemic-dt.jpg)
