Download
1 / 14
150 likes | 340 Views
Submitted by: Lindsey Fogle , MSIV Date Accepted: 25 August 2010. RAD 4001 Case Presentation. Faculty Reviewer: Sandra Oldham, M.D. Principal Modality (1): Plain film Principal Modality (2): MRI T1-weighted. 10yo boy with chronic leg pain. Plain film of left tibia and fibula. Findings.

E N D
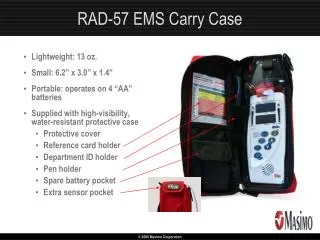
Submitted by: Lindsey Fogle, MSIV Date Accepted: 25 August 2010 RAD 4001 Case Presentation Faculty Reviewer: Sandra Oldham, M.D. Principal Modality (1): Plain film Principal Modality (2): MRI T1-weighted
10yo boy with chronic leg pain Plain film of left tibia and fibula
Findings • Radiolucent nidus in the cortex of distal tibial diaphysis • Nidus surrounded by dense osteosclerosis • Axial cut of T1 post contrast image shows well demarcated, enhancing lesion Plain film of left tibia and fibula Axial T1-weighted MRI post contrast
Differential Diagnosis • Benign bone tumors • Osteoid osteoma • Osteoblastoma • Osteochondroma • Osteofibrousdysplasia • Fibrous dysplasia • Enchondroma • 20-50yo; M=F; bones of hands/feet • Giant cell tumor • 20-40yo; F>M; epiphysis of distal femur/proximal tibia • Malignant bone tumors • Osteosarcoma • Chondrosarcoma • 30-60yo; M>F; pelvic bones/proximal femur • Ewing's sarcoma • Bone cysts • Typically appear lytic, expansile, with thin surrounding cortical bone
Osteochondroma • M>F; 10-30yo • Hamartomatous lesion resulting from a defect in the growth plate on the metaphyseal side; direct communication with medullary canal; always points away from joint of origin • Pedunculated (distal femur) or sessile (proximal humerus) • Familial form (Hereditary Multiple Exostosis) is AD with diffuse involvement • Findings: cartilaginous cap at bony base is required for diagnosis • Surgery if symptomatic only; most are assymptomatic
Osteofibrous Dysplasia • M>F; ≤ 10yo • Usually asymptomatic, but can cause anterior bowing • Suspected to be a hamartomatous process that involutes • Almost exclusively in the diaphysis of the tibia, but can occur in the fibula or bilaterally • Findings: lytic lesions surrounded by sclerosis -> “soap bubble appearance” • Treat large or symptomatic lesions with curettage and bone grafting • Fibrous dysplasia: F>M; dx typically before 30yo; Inability to produce mature lamellar bone; can be monostotic/polyostotic or polyostotic with endocrine abnormalities (McCune-Albright syndrome); also takes soap bubble appearance -> need histology to differentiate; treatment is same
Osteosarcoma (classic) • M>F; 10-25yo • Second most common primary malignancy of bone after Multiple Myeloma (20% of all primary bone malignancies) • Risk factors include Paget’s disease, Familial retinoblastoma, and radiation • Most in metaphysis of distal femur or proximal tibia; can also be in the proximal humerus • Aggressive, can metastasize to lungs • Findings: Lytic lesion that permeates giving “sunburst” appearance-> breakthrough of periostium results in “Codman triangle” • MRI indicated for staging and anatomic data for surgery • Treat with chemotherapy and surgery
Ewing’s Sarcoma • M>F; 5-25yo • Malignant bone lesion • Translocation abnormality involving chomosomes 11 and 22 in 90% of cases • Pelvis is most common location, but also seen in femur, tibia, humerus, and scapula • Typically in diaphyseal-metaphyseal region • Findings: central lytic lesion with extending destruction of cortex; takes “onionskinning” appearance from periosteal reaction • Can resemble osteomyelitis because of high grade nature, necrosis and liquefaction that occur, mistaking it for pus • Radiosensitive tumor, but current treatment also involves surgery
OsteoidOsteoma • Epidemiology • 10% of benign bone tumors; most common of the benign tumors • M>F; 5-30yo with peak incidence in 2nd decade • Most commonly in proximal femur, but also occurs in spine or tibialdiaphysis • Pathology • Osteoid forming neoplasm <1cm in diameter of benign woven bone in the nidus • Nidus contains numerous osteoblasts and osteoclasts in vascular fibrous stroma • Note: Osteoblastomas are large OsteoidOsteomas with preference for the posterior spine • Clinical Presentation • Usually assymptomatic • Night pain or dull, aching pain that is progressive • Tenderness over lesion • Classification for all benign tumors • Stage 1 – latent; generally asymptomatic; usually resolve on their own • Stage 2 – active; less well demarcated; require more aggressive treatment • Stage 3 – aggressive lesions; extensive destruction; requires wide en bloc resection • Treatment • Pain relieved by NSAIDs • High concentration of prostaglandins in nidus • 50% will “burn out” over time • If NSAIDs fail.. • CT guided radiofrequency ablation (IR) • Surgical removal (Ortho)
Typical findings of Osteoid Osteoma • Radiolucent nidus on plain film • Measures up to 1cm in diameter • Nidus surrounded by dense, reactive osteosclerosis if a cortical lesion; creates an extending fusiform bulge • Less sclerosis noted with more central lesions • Inflammatory synovitis can result if adjacent to or in a joint • Technetium bone scan is always positive • CT is helpful for anatomic data in preparing for surgery
CT-guided Radiofrequency Ablation (RFA) Axial CT without contrast images of left distal tibia and fibula
Pre- and Post-RFA Pre-treatment Post-treatment Axial T1 weighted MRI post contrast images of left distal tibia and fibula
References • Herring, William. "Chapter 21: Recognizing Abnormalities of Bone Density." Learning Radiology: Recognizing the Basics. Philadelphia: Mosby Elsevier, 2007. 217-30. Print. • Goljan, Edward F. "Chaprter 23: Musculoskeletal Disorders." Pathology. Philadelphia, PA: Mosby Elsevier, 2007. 522-26. Print. • PolouskyJohn D, Eilert Robert E, "Chapter 24. Orthopedics" (Chapter). Hay WW, Jr., Levin MJ, Sondheimer JM, Deterding RR: CURRENT Diagnosis & Treatment: Pediatrics, 19e: http://www.accessmedicine.com/content.aspx?aID=3405856. • Randall R. L, Hoang Bang H, "Chapter 6. Musculoskeletal Oncology" (Chapter). Skinner HB: CURRENT Diagnosis & Treatment in Orthopedics, 4e: http://www.accessmedicine.com/content.aspx?aID=2320059. • Srinivasan Ramesh C, Tolhurst Stephen, Vanderhave Kelly L, "Chapter 40. Orthopedic Surgery" (Chapter). Doherty GM: CURRENT Diagnosis & Treatment: Surgery, 13e: http://www.accessmedicine.com/content.aspx?aID=5314010. • ZeigerRoni F, McGraw-Hill's Diagnosaurus 2.0: http://www.accessmedicine.com/diag.aspx Special thank you to M.D. Anderson Cancer Center for patient’s images.