Download
1 / 103
1.04k likes | 1.37k Views
BIOMATERIALS AND ARTIFICIAL ORGAN BM1303 S.Sudha Lecturer Dept of Biomedical Engg. UNIT I . INTRODUCTION TO BIOMATERIALS. During the last two decades, significant advances have been made in thedevelopment of biocompatible and biodegradable materials for medicalapplications.

E N D
BIOMATERIALS AND ARTIFICIAL ORGANBM1303S.SudhaLecturer Dept of Biomedical Engg
INTRODUCTION TO BIOMATERIALS • During the last two decades, significant advances have been made in thedevelopment of biocompatible and biodegradable materials for medicalapplications. • In the biomedical field, the goal is to develop and characterize artificial materialsor, in other words, “spare parts” for use in the human body to MEASURE,RESTORE and IMPROVE physical functions and enhance survival and qualityof life.
What’s a biomaterial? • 1980 - Passive and inert point of view Any substance or drugs, of synthetic or natural origin, which can be used for any period alone or as part of a system and that increases or replaces any tissue,organ or function of the body • 1990 – Active point of view Non-living material used in a medical device and designed to interact with biological systems
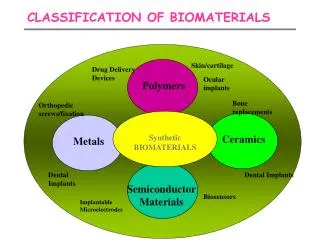
Classification of biomaterials First generation: INERT Do not trigger any reaction in the host: neither rejected nor recognition “do not bring any good result” Second generation: BIOACTIVE Ensure a more stable performance in a long time or for the period you want Third generation: BIODEGRADABLE It can be chemically degraded or decomposed by natural effectors (weather, soil bacteria, plants, animals)
What is a biocompatible material? • Synthetic or natural material used in intimate contact with living tissue (it canbe implanted, partially implanted or totally external). • Biocompatible materials are intended to interface with biological system toEVALUATE, TREAT, AUGMENT or REPLACE any tissue, organ or function ofthe body. • A biocompatible device must be fabricated from materials that will not elicit an adverse biological response
Mechanical Properties of Metals How do metals respond to external loads? Stress and Strain • Tension • Compression • Shear • Torsion Elastic deformation Plastic Deformation • Yield Strength • Tensile Strength • Ductility • Toughness • Hardness
Stress-Strain Behavior Elastic deformation • Reversible: when the stress • is removed, the material • returns to the dimension it • had before the loading. • Usually strains are small • (except for the case ofplastics). Plastic deformation • Irreversible: when the stress • is removed, the material • does not return to its • previous dimension.
Stress-Strain Behavior: Plastic deformation • Plastic deformation: stress and strain are not proportional the deformation is not reversible deformation occurs by breaking and rearrangement of atomic bonds (in crystalline materials primarily by motion of dislocations)
Typical mechanical properties of metals The yield strength and tensile strength vary with prior thermal and mechanical treatment, impurity levels, etc. This variability is related to the behavior of dislocations in the material. But elastic moduli are relatively insensitive to these effects. The yield and tensile strengths and modulus of elasticity decrease with increasing temperature, ductility increases with temperature.
Mechanics of Materials • The point up to which the stress and strain are linearly related is called the proportional limit. • The largest stress in the stress strain curve is called the ultimate stress. • The stress at the point of rupture is called the fracture or rupture stress. • The region of the stress-strain curve in which the material returns to the undeformed state when applied forces are removed is called the elastic region. • The region in which the material deforms permanently is called the plastic region. • The point demarcating the elastic from the plastic region is called the yield point. The stress at yield point is called the yield stress.
Mechanics of Materials • The permanent strain when stresses are zero is called the plastic strain. • The off-set yield stress is a stress that would produce a plastic strain corresponding to the specified off-set strain. • A material that can undergo large plastic deformation before fracture is called a ductile material. • A material that exhibits little or no plastic deformation at failure is called a brittle material. • Hardness is the resistance to indentation. • The raising of the yield point with increasing strain is called strain hardening. • The sudden decrease in the area of cross-section after ultimate stress is called necking.
Viscoelasticity Definition: time-dependent material behavior where the stress response of that material depends on both the strain applied and the strain rate at which it was applied! Examples • biological materials • polymer plastics • metals at high temperatures
Elastic versus viscoelastic behaviors For a constant applied strain • An elastic material has a unique material response • A viscoelastic material has infinite material responses depending on the strain-rate
Viscoelastic Hysteresis Viscoelastic solid • some energy is dissipated with dashpots (as heat)some energy is stored in springs. Area in the hysteresis loop is a function of loading rate • For viscoelastic material, energy is dissipated regardless of whether strains(or stresses) are small or large • Under repetitive loading, a viscoelastic material will heat up
Wound healing • All wounds heal following a a specific sequence of phases which may overlap • The process of wound healing depends on the type of tissue which has been damaged and the nature of tissue disruption • The phases are: • Inflammatory phase • Proliferative phase • Remodelling or maturation phase
The ways in which wounds heal Three basic classifications exist: • Healing by primary intention Two opposed surfaces of a clean, incised wound (no significant degree of tissue loss) are held together. Healing takes place from the internal layers outwards • Healing by secondary Intention If there is significant tissue loss in the formation of the wound, healing will begin by the production of granulation tissue wound base and walls. • Delayed primary healing If there is high infection risk – patient is given antibiotics and closure is delayed for a few days e.g. bites
Wound assessment Lab tests: TcPO2 Signs of infection Size, depth & location Odour or exudate WOUND ASSESSMENT • Wound bed: • necrosis • granulation Wound edge Surrounding skin: colour, moisture,
The healing process • Day 0 – 5 • The healing response starts at the moment of injury – the clotting cascade is initiated • This is a protective tissue response to stem blood loss • The inflammatory phase is characterised by heat, swelling, redness, pain and loss of function at the wound site • Early (haemostasis) • Late (phagocytosis) • This phase is short lived in the absence of infection or contamination
Granulation • Day 3 – 14 • Characterised by the formation of granulation tissue in the wound • Granulation tissue consists of a combination of cellular elements including: • Fibroblasts, inflammatory cells, new capillaries embedded in a loose extra-cellular collagen matrix, fibronectin and hyularonic acid
Moist wound healing • Basic concept is that the presence of exudate will provide an environment that stimulates healing • Exudate contains: • Lysosomal enzymes, WBC’s, Lymphokines, growth factors…….. • There are clinical studies which have shown that wounds maintained in a moist environment have lower infection rates and heal more quickly
Factors affecting healing • Immune status • Blood glucose levels (impaired white cell function) • Hydration (slows metabolism) • Nutrition • Blood albumin levels (‘building blocks’ for repair, colloid osmotic pressure - oedema) • Oxygen and vascular supply • Pain (causes vasoconstriction) • Corticosteroids (depress immune function)
Host Reactions to Biomaterials • Effect of the Implant on the Host • Local • Blood material interactions • Protein adsorption • Coagulation • Fibrinolysis • Platelet adhesion, activation, release • Complement activation • Leukocyte adhesion, activation • Hemolysis • Toxicity
Modification of normal healing • Encapsulation • Foreign body reaction • Pannus formation • Infection • Tumorgenesis • Systemic and remote • Embolization • Hypersensitivity • Elevation of implant elements in the blood • Lymphatic particle transport
Effect of the Host on the Implant • Physical – mechanical effects • Abrasive wear • Fatigue • Stress corrosion, cracking • Corrosion • Degeneration and dissolution • Biological effects • Absorption of substances from tissues • Enzymatic degradation • Calcification
Activated by injury to vascularized connective tissue • Series of reactions • Various cells • Controlled by endogenous and autocoid mediators
Types of Metallic Implants • Stainless steel • Cobalt Based Alloys • Titanium Alloys
Stainless Steels • Fe 60-65 wt%, Cr 17-19 wt %, Ni 12-14 wt% • Carbon content reduced to 0.03 wt% for better The most common stainless steel: 316Lresistance to in vivo corrosion. • Why reduce carbon: Reduce carbide (Cr23C6) formation at grain boundary. Carbide impairs formation of surface oxide • Why add chromium: corrosion resistance by formation of surface oxide. • Why add nickel: improve strength by increasing face centered cubic phase (austenite)
Stainless Steels Good stainless steel: • Austenitic (face centered cubic) • No ferrite (body centered cubic) • No carbide • No sulfide inclusions • Grain size less then 100mm • Uniform grain size
Cobalt Based Alloys Common types for surgical applications: • – ASTM F75 • – ASTM F799 • – ASTM F790 • – ASTM F 562
Cobalt Alloys: ASTM F75 • Co-Cr-Mo • Surface oxide; thus corrosion resistant • Wax models from molds of implants • Wax model coated with ceramic and wax melted away • Alloy melted at 1400 °C and cast into ceramic molds.
Cobalt Alloys: ASTM F75 Three caveats: • – Carbide formation ® corrosion. Solution: annealing at 1225 °C for one hour. • – Large grain size ® reduced mechanical strength • – Casting defects ® stress concentration, propensity to fatigue failure
Cobalt Alloys: ASTM F799, ASTM F90 Cobalt Alloys: ASTM F799 • Modified form of F75: hot forged after casting • Mechanical deformation induces a shear induced transformation of FCC structure to HCP. • Fatigue, yield and ultimate properties are twice of F75. Cobalt Alloys ASTM F90 : • W and Ni are added to improve machinability and fabrication • Mechanical properties similar to F75 • Mechanical properties double F75 if cold worked
Titanium Based Alloys • Lighter • Good mechanical properties • Good corrosion resistance due to TiO2solid oxide layer • Ti-6% wt Al-4% wt V (ASTM F136) is widely used • Contains impurities such as N, O, Fe, H, C • Impurities increase strength reduce ductility
Titanium Alloys: ASTM F136 • HCP structure transforms to BCP for temperatures greater than 882 °C. • Addition of Al stabilizes HCP phase by increasing transformation temperature • V has the inverse effect.
ceramic • Any of various hard, brittle, heat-resistant and corrosion-resistant materials made by shaping and then firing a nonmetallic mineral,such as clay, at a high temperature • Clinical success requires: Achievement of a stable interface with connective tissue Functional match of the mechanical behavior of the implant with the tissue to be replaced • Critical Issues: Integrity of bioceramic Interaction with the tissue
Hydroxyapatites (HA) • Chemically similar to mineral component of bones • It will support bone ingrowth and osseointegration • when used in orthopaedic, dental and maxillofacial applications • Chemical formula: Ca5(PO4)3OH • Hexagonal Bravais lattice • The chemical nature of hydroxyapatite lends itself to substitution; common substitutions involve carbonate, fluoride and chloride substitutions for hydroxyl groups
Uses for HA • Facial augmentation with hydroxyapatite has been used for the following corrections: Cheek, Chin, Jaw, Nose, Browbone. • Skeletal repair biomaterials • Ocular prosthesis • Hydroxyapatite from coral • The eye muscles can be attacheddirectly to this implant, allowing it to move within the orbit-just like the natural eye.
Calcium Phosphate Bioceramics • There are several calcium phosphate ceramics that are consideredbiocompatible; most are resorbable and will dissolve when exposed tophysiological environments. • Hydroxyapatite is thermodynamically stable at physiological pH values; actively takes part in bone bonding, forming strong chemical bonds with surrounding bone • Mechanical properties unsuitable for load-bearing applications such as orthopaedics • Used as a coating on materials such as titanium and titanium alloys,where it can contribute its 'bioactive' properties, while the metallic component bears the load • Coatings applied by plasma spraying
Polymeric Biomaterials • What is a polymer? Long chain molecules that consist of a number of repeating units (mers) Fabricated from monomers which change somehow in polymerization Loss of H20, HCl or other molecule • Polymer properties are more complex than for simpler materials Types of polymers Biological polymers • DNA, cellulose, starch, proteins, rubber, etc • Often reconstituted to form usable polymer • Mainly collected from animals Synthetic polymers • Fabricated from petroleum products (generally) • May be also a modified biological polymer • Most plastics and similar materials
Classification examplesexamplesexamples Polymers Thermosets Thermoplastics Elastomers or Rubbers
Classes of Polymers (I) • Thermoplastic polymers: • Long chains with very limited or no cross-linking • They behave in a plastic, ductile manner (above Tg) • Melt when heated and are thus easily remolded and recycled • Thermoset polymers: • Highly cross-linked, 3D network structures • Generally brittle (at most temperatures) • Decompose when heated and can’t easily be reshaped or recycled
Classes of Polymers (II) Elastomers and rubbers Large amounts of elastic deformation Some (light) cross-linking Typically, about 1 in 100 molecules are cross-linked on average Average number of cross-links around 1 in 30 yields a more rigid and brittle material (closer to a thermoset) Crosslinks allows material to return to original shape without plastic deformation elastomer thermoset
Definitions • Oligomer- molecules with n<10 (less than ten monomers) • Degree of polymerization, P= number of monomer residues per chain • Functionality: number of bonding sites per monomer.A monomer must possess at least two bonding sites • Homopolymer A-A-A-A-A-A-A-A • Copolymer Random : A-B-A-A-A-B-B-A-B-B-B-A-B-B Alternating : A-B-A-B-A-B-A-B-A-B Block : A-A-A-A-A-B-B-B-B-B-B Graft A’s with B’s on branches • Linear polymer- no branches • Branched polymer - multiple branches • Crosslinked polymer- links between branches
Polymer Basics • Polymerization process: • Initiation: I → 2R• (the active center which acts as a chain carrier is created) • Propagation: RM1• + M → RM2• (growth of macromolecular chain) • Termination: kinetic chain is brought to halt
Synthesis Reactions: • Addition polymerization • Condensation polymerization • Source: Askeland & Phule p 677