Download
1 / 28
310 likes | 692 Views
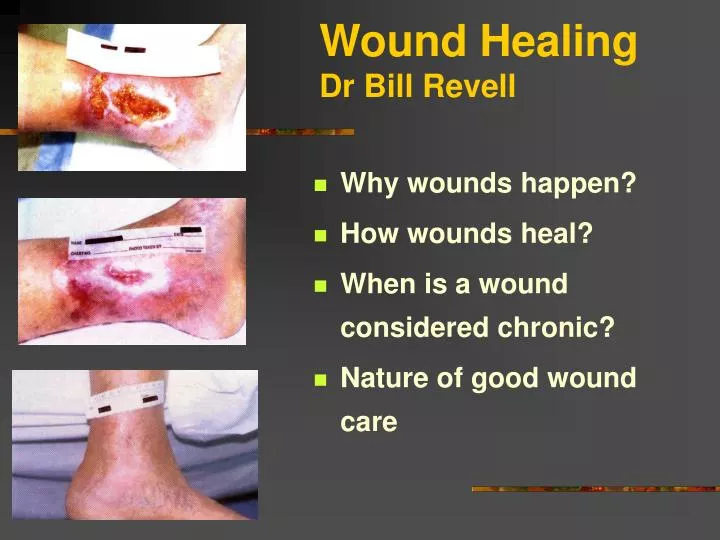
Wound Healing Dr Bill Revell. Why wounds happen? How wounds heal? When is a wound considered chronic? Nature of good wound care. Wound healing. Restoration of the normal anatomic continuity to a disrupted area of tissue Wounds: Clean Contaminated

E N D
Wound HealingDr Bill Revell • Why wounds happen? • How wounds heal? • When is a wound considered chronic? • Nature of good wound care
Wound healing • Restoration of the normal anatomic continuity to a disrupted area of tissue • Wounds: • Clean • Contaminated • Infected (>105 bacteria per gram of tissue)
Why do wounds happen? • Basic underlying causes must be identified and controlled before healing is begun • Trauma (initial, repetitive) • Scolds/burns (physical and chemical) • Animal bites/insect stings • Pressure • Vascular compromise • Immunodeficiency • Connective tissue disorders • Metabolic disease (including diabetes) • Nutritional deficiencies • Psychosocial disorders • Adverse effects of medications
Often multifactorial • Ulcer • Lower leg oedema • Drains copious amount of fluid • irritates skin • Incapacitated • sits all day • worsens oedema
Pressure ulcer surrounded by erythema • Spinal cord injured patient • Chronic pressure ulcer • Erythema • Infection? • Irritation of wound fluid? • Incontinence? • Continual pressure?
How do wounds heal? • Haemostasis • Inflammation • These two phases often combined as “inflammatory phase” • Proliferation • Remodelling or maturation
PMN – Poly Morpho Nucleocytes Neutrophils Basophils Eosinophils
1. Haemostasis • Platelets – key role in forming stable clot • Also constriction of blood vessels • spasm ultimately relaxes • ADP leaks from damaged tissues • platelets aggregate and adhere to exposed collagen • secrete cytokines (eg PDGF)………
………. blood clotting • Intrinsic clotting cascade • Production of thrombin • Initiates production of fibrin • (from prothrombin) • Fibrin mesh strengthens platelet aggregate into stable haemostatic plug • Platelets also secrete cytokines (eg PDGF) • factors involved in initiating cascade • Haemostasis usually within minutes
2. Inflammation • Local vasodilatation; Fluid leakage in extra vascular space; Blockage of lymphatic drainage • Rubor (redness) • Tumour swelling) • Calor (heat) • Dolor (pain) – produced by distension of tissue spaces from swelling, and by chemical irritation of nociceptors) • Swelling and pain loss of function Rubor et tumour cum calore et dolore
Inflammation (up to 4 days) • “Clean up the debris” • Leaky blood vessel plasma and neutrophils to surrounding tissue • Neutrophils phagocytose debris and microorganisms • aided by local mast cells • as fibrin breaks down, degradation products attract the next cell involved erythema
Macrophage direction……… • Macrophages also phagocytose undesirable elements • Also………… • Secrete variety of chemotactic (eg fibronectin) and growth factors (including angiogenic factors) • Fibroblast growth factor (FGF) • Epidermal growth factor (EGF) • Transforming growth factor beta (TGF) • Interleukin-1 (IL-1) • Which direct the next stage……………
3. Proliferative phase (proliferation, granulation, wound contraction) • 4 – approx 21 days • Pebbled red tissue in wound base • Replacement of dermal tissues (sometimes subdermal) • Wound contraction
Proliferation phase (rebuild structure) • Fibroblasts • Collagen framework on which further dermal regeneration occurs • Angiogenesis • Pericytes outer lining of blood vessels • Endothelial cells inner vessel layer • Keratinocytes • Re-epithelialisation • some differentiate to form protective outer layer (stratum corneum) – final stage contracture
Re-epithelialisation: concurrent with formation of granulation tissue • Reformation of epithelial (epidermal) sheet • Basal keratocytes switch to migratory phenotype • Secrete connective tissue degrading enzymes; facilitate movement across newly deposited or exposed extracellular matrix • Granulation tissue rapidly covered • Reformed epidermis source of growth factors eg IL-1, TGF-1
Scar following wound healing • Red, immature; mature, normal skin colour • May develop fibrous bands, nonpliable • May be painful, itchy • Contracture may develop as scar heals (myofibroblasts) • Scar from larger, deeper wounds may become raised above skin level (collagen +++) hypertrophic scar • Greater response in dark skin
Keloid scars • Hypertrophic scars larger than original wound • Most common in dark skin
4. Remodelling • Remodelling dermal tissues to produce greater tensile strength • Deposition of matrix materials • Fibronectin, hyaluronic acid, proteoglycans and collagen serve as scaffold for cellular migration and tissue support • ….and subsequent changes over time • Up to 2 years after wounding • Collagen: max level 2-4 weeks post injury • Tensile strength 40% pre-injury strength 1 month post-injury; increased up to a year • Never >80% • Apparently healed wounds can break down dramatically if attention not paid to initial causative factors
When is a wound considered chronic? • Healthy individuals - acute wound should heal within 3/52… remodelling for next year or so • Wound may become stuck in one of the stages….. wound becomes chronic • Definition: “wounds which have failed to proceed through an orderly and timely process to produce anatomic and functional integrity, or proceeded through the repair process without establishing a sustained anatomic and functional result” • Lazarus G et al (1994). Arch. Derm 130: 489-493
Kloth LC and McCullock (2002). Wound healing; alternatives in management
Kloth LC and McCullock (2002). Wound healing; alternatives in management
Principles of Good Chronic Wound Care • Identify and control the underlying causes • Support patient centred concerns • Optimise local wound care
Occlusive, moist dressings……… • Decreased dehydration and cell death • Increased angiogenesis • Enhanced autolytic debridement • Increased re-epithelialisation • Bacterial barrier and decreased infection rates • Decreased pain • Decreased costs
Occlusive moist dressings and wound healing • Decreased dehydration and cell death • Activity of neutrophils, macrophages, fibrocytes, pericytes etc. Cannot function in a dry environment • Increased angiogenesis • Cells need moist environment; also, occurs in regions of low PO2. Occlusive dressings may act as stimulus • Enhanced autolytic debridement • Neutrophil cell life is prolonged, and proteolytic enzymes carried to wound bed painless debridement. Fibrin degradation products are a factor in stimulating macrophages to release growth factors into wound bed
Occlusive moist dressings and wound healing: • Increased re-epithelialisation • epidermal cells must spread over wound surface from edges; need blood and nutrients. Dry, crusted wounds reduce supply and provide a barrier to migration • Bacterial barrier and decreased infection rates • Occlusive dressings can provide a barrier to microorganism migration wound. • Decreased pain • Moist bed insulates and protects nerve endings. Occlusive dressings often requires less changes ……………….but how moist is moist?