Download
1 / 58
580 likes | 665 Views
2008 Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents : Part 1. Major Changes Since 2008.

E N D
2008 Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents : Part 1
Major Changes Since 2008 (1) more emphasis on the importance of ART for prevention and treatment of OIs, especially those for which specific chemoprophylaxis and treatment do not exist; (2) information on diagnosis and management of immune reconstitution inflammatory syndromes (IRIS); (3) information on interferon-gamma release assays (IGRAs) for the detection of latent Mycobacterium tuberculosis infection;
Major Changes Since 2008 (4) updated information on drug interactions affecting use of rifamycin drugs for prevention and treatment of tuberculosis (TB); (5) the addition of a section on hepatitis B virus (HBV) infection; (6) the addition of a section on malaria to the OIs of geographic interest.
Initiation of ART in the Setting of an Acute OI (Treatment-Naïve Patients) No consensus has been reached concerning the optimal time to start ART in the setting of a recently diagnosed OI. Recently completed RCT demonstrated a clinical and survival benefit of starting ART early, within the first 2 weeks, of initiation of treatment for an acute OI, excluding TB Zolopa A, et al., ACTG A5164. 15th CROI; 2008; Boston, MA. Abstract 142.
Initiation of ART in the Setting of an Acute OI (Treatment-Naïve Patients) • Majority of OIs represented were PCP and serious bacterial infections • Study Conclusion • Unless there are other contraindications, early initiation of ART near the time of initiation of OI treatment should be considered for most patients with an acute OI, excluding TB. Zolopa A, et al., ACTG A5164. 15th CROI; 2008; Boston, MA. Abstract 142.
Initiation of ART in the Setting of an Acute OI (Treatment-Naïve Patients) In cases of cryptosporidiosis, microsporidiosis, PML, KS, PCP, and serious bacterial infections, the early benefits of ART outweigh increased risk related to these other factors and ART should be started as soon as possible Risks of early ART initiation may be greatest in those with CNS IRIS leading to increased ICP and brain shift (WCM opinion) Zolopa A, et al., ACTG A5164. 15th CROI; 2008; Boston, MA. Abstract 142.
Management of Acute OIs in Patients Receiving ART: 3 Groups • OIs that occur shortly after initiating ART (within 12 weeks). • “unmasking” IRIS • Treat OI and continue ART • OIs occurring >12 weeks after initiation of ART among patients with suppressed pVL and CD4+ >200 cells/μL • IRIS vs incomplete immune restoration • Continue ART • No evidence that changing the ART regimen in this setting will improve the CD4+ response • OIs that develop in setting of virologic and immunologic failure while on potent ART • Treat OI • HIV resistance testing and regimen change
Special Considerations During Pregnancy For pregnant women who have had an OI diagnosed and are not on ART, immediate initiation of ART with OI therapy should be encouraged to minimize the risk of perinatal transmission of HIV. Decisions about immediate versus delayed initiation of ART in pregnancy should take into account gestational age, maternal HIV RNA levels and clinical condition, and potential toxicities and interactions between ART and OI drugs.
Pneumocystis Pneumonia • Epidemiology • 90% of cases with CD4+ counts of <200 cells/μL • Other risk factors • CD4+ cell percentage <14% • previous episodes of PCP • oral thrush • recurrent bacterial pneumonia • unintentional weight loss • higher plasma HIV RNA • Mortality 20%–40% with profound immunosuppression
Pneumocystis Pneumonia • Clinical Manifestations • subacute onset of progressive dyspnea, fever, nonproductive cough, and chest discomfort • Chest clear or “cellophane” rales • Oxygenation variable • LDH >500 mg/dL is common but nonspecific
Pneumocystis Pneumonia • CXR typically bilateral interstitial infiltrates or normal (if mild) • Atypical presentations: nodules, blebs and cysts, asymmetric disease, upper lobe localization, and pneumothorax occur. • Pneumothorax in a patient with HIV infection should raise the suspicion of PCP • Cavitation, intrathoracic adenopathy, and pleural effusion are uncommon • presence might indicate an alternative diagnosis. • Approximately 13%–18% of patients with documented PCP have another concurrent cause of pulmonary dysfunction (e.g., TB, KS, or bacterial pneumonia)
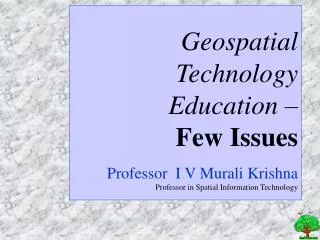
PCP Severe Pneumocystis Pneumonia
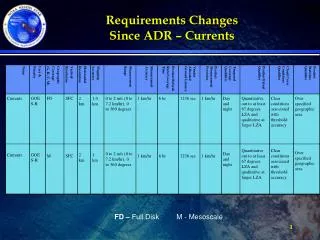
Pneumocystis Pneumonia: Diagnosis • Expectorated sputum not useful • Sensitivity of • induced sputum <50%–>90% • bronchoalveolar lavage 90%–99% • transbronchial biopsy 95%–100% • open lung biopsy 95%–100% • Methods • Giemsa, Diff-Quik, and Wright stains • Gomori methenamine silver (GMS) • IFA • PCR sensitive but not specific • Other • S-adenosylmethionine (which is lowered in cases of active PCP) • (1→3)ß-D-glucan (levels increase with PCP)
Geimsa: left GMS: below
Pneumocystis Pneumonia: Treatment • Initiate presumptive treatment without delay • TMP-SMX is the treatment of choice • Adjunctive corticosteroids • pO2 <70 mm Hg or Aa O2 gradient >35 mm Hg RA within 72 hours of starting PCP treatment • Reduce Mortality about 50% • “Rescue” steroids (after 72 h) of uncertain benefit • Ventilatory support • survival in up to 50% requiring ventilatory support
Pneumocystis Pneumonia: Treatment • Many health care providers delay initiation of ART until after the completion of anti-PCP therapy, or until at least 2 weeks after initiating anti-PCP therapy • Additive/synergistic toxicities • Rare IRIS
Pneumocystis Pneumonia: Treatment Failure Important to wait at least 4–8 days before switching therapy for lack of clinical improvement In the absence of corticosteroid therapy, early and reversible deterioration within the first 3–5 days of therapy is typical Failure due to lack of drug efficacy occurs in approximately 10% of those with mild-to-moderate disease Other concomitant infections must be excluded (BAL) use parenteral pentamidine or primaquine combined with clindamycin for moderate-severe disease
Pneumocystis Pneumonia: Toxicity Management • Treatment-limiting toxicities occurs in up to one-third of patients • TMP-Sulfa • rash (30%–55%) (including SJS) • fever (30%–40%) • leukopenia (30%–40%) • thrombocytopenia (15%) • azotemia (1%–5%) • hepatitis (20%) • hyperkalemia.
Pneumocystis Pneumonia: Toxicity Management • Pentamidine (IV) • azotemia, pancreatitis, hypo- or hyperglycemia, leukopenia, electrolyte abnormalities,hypotension during infusion, and cardiac dysrhythmia • Dapsone and Primaquine • Hemolysis with G6PD deficiency • Methemoglobinemia
Pneumocystis Prevention • Primary prophylaxis • CD4+ count of <200 cells/μL or a history of oropharyngeal candidiasis • CD4+ cell percentage of <14% or a history of an AIDS-defining illness • Discontinuing primary prophylaxis • response to ART with increase CD4+ counts to >200 cells/μL for >3 months • reintroduced if the CD4+ count decreases to <200 cells/μL • Secondary prophylaxis • chronic maintenance therapy with TMP-SMX unless immune reconstitution occurs as a result of ART • discontinued when CD4+ count increased from <200 cells/μL to >200 cells/μL for >3 months as a result of ART • If the episode occurred at a CD4+ count of ≥200 cells/μL, continue PCP prophylaxis for life
Toxoplasma Encephalitis (TE) • Epidemiology • Seroprevalence 15% in the United States and 50%–75% in certain European countries • Greatest risk with a CD4+ count <50 cells/μL • Rare if CD4>200 • 12 month incidence if not receiving prophylaxis with drugs active against T. gondii approximately 33% • incidence of toxoplasmosis in patients who are seronegative for Toxoplasma is extremely low
TE: Clinical Manifestations Focal encephalitis with headache, confusion, or motor weakness and fever CT scan or MRI of the brain will typically show multiple contrast-enhancing lesions, often with associated edema Can manifest as single lesions, especially by CT
TE: Diagnosis • Almost uniformly seropositive for anti-toxoplasma IgG in serum • Absence of IgG antibody makes a diagnosis of toxoplasmosis unlikely but not impossible • Detection of T. gondii by PCR in CSF disappointing • Specificity is high (96%–100%), • Sensitivity is low (50%) and the • Usually negative once specific anti-toxoplasma therapy started
TE: Differential Diagnosis • Primary CNS lymphoma • CD4 < 50 • Tuberculomas • Fungal infection (e.g., cryptococcosis) • Chagas disease • Bacterial abscess • rarely PML (inflammatory form) • Neurocysticercosis
TE: Prevention • Primary • test for IgG antibody to Toxoplasma soon after the diagnosis of HIV infection to detect latent infection with T. gondii • advise not to eat raw or undercooked meat, including undercooked lamb, beef, pork, or venison • avoid cat litter • Toxoplasma-seropositive patients who have a CD4+ count of <100 cells/μL should be administered prophylaxis against TE (TMP-SMX)
TE: Prevention • Discontinuing Primary Prophylaxis • patients who have responded to ART with an increase in CD4+ counts to >200 cells/μL for >3 months • reintroduced if the CD4+ count decreases to <100–200 cells/μL
TE: Treatment Initial therapy of choice for TE consists of the combination of pyrimethamine plus sulfadiazine plus leucovorin Some treat severely ill patients initially requiring parenteral therapy for TE with parenteral TMP-SMX (oral pyrimethamine could be considered in addition to IV TMP-SMX) or oral pyrimethamine plus parenteral clindamycin
TE: Treatment Acute therapy for TE should be continued for at least 6 weeks, if there is clinical and radiologic improvement Adjunctive corticosteroids (dexamethasone) only for treatment of a mass effect or associated edema Anticonvulsants should not be administered as prophylactics to all patients
TE: Treatment Failure • A brain biopsy should be strongly considered for patients who fail to respond to initial therapy for TE • defined by clinical or radiologic deterioration during the first week despite adequate therapy OR • lack of clinical improvement within 2 weeks.
TE: Secondary Prophylaxis Pyrimethamine plus sulfadiazine plus leucovorin is highly effective as suppressive therapy for patients with TE For sulfa intolerant patients, pyrimethamine plus clindamycin TMP-SMX could be used as a suppressive regimen to reduce pill burden1 1. Duval, X et al., AIDS, 2004. 18(9): p. 1342-4.
TE: Secondary Prophylaxis • Discontinuing maintenance therapy • Consider if sustained increase in their CD4+ counts of >200 cells/μL after ART (e.g., >6 months) • Reintroduced if the CD4+ count decreases to <200 cells/μL
dMAC: Epidemiology • Ubiquitous in the environment • The mode of transmission: inhalation, ingestion, or inoculation via the respiratory or gastrointestinal tract • MAC disease generally occurs among persons with CD4+ counts <50 cells/μL (20-40%) • Overall incidence rate 2 cases per 100 person-years among those with • CD4+ count <100 cells/μL receiving effective prophylaxis or • have responded to ART with a sustained increase in CD4+ count to levels >100–200 cells/μL
dMAC: Clinical Manifestations • No ART • Disseminated, multi-organ, mycobacteremia • Fever, night sweats, weight loss, fatigue, diarrhea, and abdominal pain • On ART • Localized (cervical or mesenteric lymphadenitis, pneumonitis, pericarditis, osteomyelitis, skin or soft tissue abscesses, genital ulcers, or CNS infection)
dMAC: Clinical Manifestations • Disseminated • Anemia • Increased alkaline phosphatase • Hepatomegaly • Splenomegaly • Lymphadenopathy
MAC IRIS Focal lymphadenitis with fever Absent mycobacteremia
dMAC: Diagnosis Isolation of MAC from cultures of blood, lymph node, bone marrow, or other normally sterile tissue or body fluids
dMAC: Prevention Chemoprophylaxis against disseminated MAC disease if CD4+ count of <50 cells/μL Primary MAC prophylaxis should be discontinued when response to ART with an increase in CD4+ counts to >100 cells/μL for ≥3 months Reintroduced if the CD4+ count decreases to <50 cells/μL