Download
1 / 36
400 likes | 614 Views
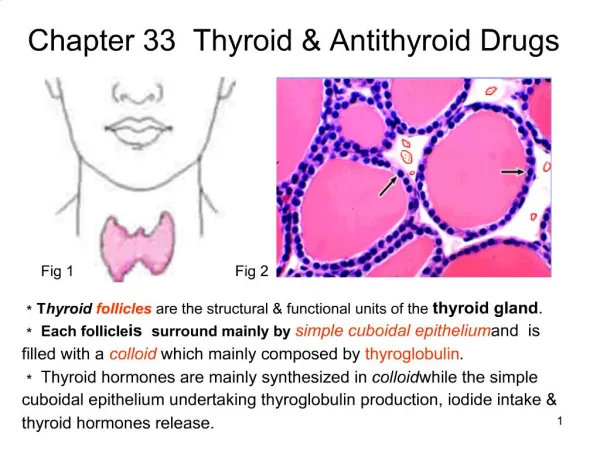
Thyroid and Anti thyroid drugs. Role of the Thyroid gland. participates in normalizing growth and development and energy levels and the proper functioning and maintenance of tissues / organs critical for the nervous, skeletal and reproductive tissues

E N D
Role of the Thyroid gland participates in normalizing growth and development and energy levels and the proper functioning and maintenance of tissues / organs critical for the nervous, skeletal and reproductive tissues it affects secretion and degradation rates of all hormones
Function of the Thyroid Gland secretion of the following hormones: triiodothyronine (T3) ; 59% iodine tetraiodothyronine (T4; also known as thyroxine); 65% iodine calcitonin
THYROID PHYSIOLOGY • Iodide Metabolism • The recommended daily adult iodide (I-) intake is 150 mcg • Biosynthesis of Thyroid Hormones • Transport of Thyroid Hormones • thyroxine-binding globulin (TBG) • about 0.04% of total T4 and 0.4% of T3 exist in the free form.
Steps in Biosynthesis • Iodide trapping • Oxidation of iodide to iodine • Iodide Organification • Formation of T4 and T3 • Release of T4 and T3
Peripheral metabolism of thyroid hormones • The primary pathway for the peripheral metabolism ofthyroxine (T4) is deiodination deiodination of T4 may occur by monodeiodination of the outer ring, producing 3,5,3'-triiodothyronine (T3), which is three to four timesmore potent than T4
Basic pharmacology of thyroid & antithyroid drugsThyroid hormones • A model of thyroid hormone action is depicted in Figure 38-4 Figure38-4. Regulation of transcription by thyroid hormones • T3 and T4 are triiodothyronine and thyroxine, respectively. • PB, plasma binding protein; • F, transcription factor; R, receptor; PP, proteins that bind at the proximal promoter.
Hypothyroidism A syndrome resulting from a deficiency of thyroid hormones and is manifested largely by a reversible slowing down of all body functions. There is a striking retardation of growth and development. In children, manifested as dwarfism and severe MR.
Synthetic Thyroid Hormone synthetic levothyroxine (syntheticT4) Brand names: Eltroxin , Euthyrox,Levoxyl, Levothroid, Synthroid for hormone replacement therapy in hypothyroidism DOSE Infants and Children require more T4/Kg body weight than adults Average dose for an infant -10-15 micrograms/kg/d Average dose for an adult – 1.7micrograms/kg/d Once daily Pharmacokinetics should be taken 30min before or 1 hour after meals (delayed absorption for soy, other foods and drugs) takes 6-8 weeks to reach steady state levels Labs should be repeated after 2 months
Synthetic Thyroid Hormone reasons for its use: stability content uniformity low cost lack of allergenic foreign protein easy laboratory measurements of serum levels long half-life (7days) once a day dosing
Synthetic Thyroid Hormone Uses Hormone replacement therapy In young patients or those with mild disease- full replacement therapy started In older patients and in patients with cardiac disease -start treatment with reduced dosage Myxedema Coma – medical emergency Loading dose –of T4 – 300-400micrograms I/V initially f/by `50micrograms daily I/V T3 – more cardiotoxic and difficult to moniter Hypothyroidism and Pregnancy – daily dose –adequate
Synthetic Thyroid Hormone synthetic liothyronine (synthetic T3) is 3-4x more potent (Cytomel,Triostat) not used alone for long term treatment secondary to short half life and large peaks in serum T3 levels increase risk for cardiac side effects secondary to hyperthyroid states during treatment
Hyperthyroidism A thyroid disorder caused by an antibody-mediated auto-immune reaction, but the trigger for this reaction is still unknown most common cause of hyperthyroidism
Anti-thyroid Drugs Thioamides Iodides radioactive iodine Beta adrenoceptor blocking agents
Thioamides Methimazole Propylthiouracil (PTU) Carbimazole MOA: inhibit synthesis by acting against iodide organification (both) coupling of iodotyrosines (both) Blocks peripheral conversion of T4 to T3 (PTU)
Thioamides Pharmacokinetics: almost completely absorbed in the GIT serum half life: 90mins(PTU) ; 6 hours (methimazole) excretion: kidney – 24 hours (PTU) ; 48 hours (Methimazole) can cross placental barrier (lesser with PTU) Methimazole 10x more potent than PTU PTU more protein-bound
Thioamide uses • Definitive therapy • Graves disease • Toxic nodular goitre • Preoperatively • In thyrotoxic patients • Along with RAI
Thioamides Adverse Effects: maculopapular rash benign transient leukopenia agranulocytosis hepatitis (PTU) ; cholestatic jaundice (Methimazole) vasculitis lupus-like syndrome
Iodine131 preparations: sodium iodide 131 MOA: trapped within the gland and enter intracellularly and delivers strong betaradiations destroying follicular cells Penetration range-400-2000µm Clinical uses: Grave’s, primary inoperable thyroid CA Contraindication: pregnancy
Iodine131 Advantages Easy administration Effectiveness Low expense Absence of pain
Iodine131 Thioamides should be given initially and stop 5-7 days before radioactive iodine administration 131I dosage generally ranges between 80-120uCi/g of estimated thyroid wt. corrected for uptake. May be repeated after 6 months Adverse effects permanent hypothyroidism potential for genetic damage may precipitate thyroid crisis
Anion Inhibitors Monovalent anions such as perchlorates, pertechnetate and thiocyanate can block uptake of iodide by the gland by competitive inhibition can be overcome by large doses of iodides useful for iodide-induced hyperthyroidism (amiodarone-induced hyperthyroidism) rarely used due to its association with aplastic anemia
Inorganic Iodines major anti-thyroids before the introduction of thioamides (1950s) preparations: strong iodine solution (Lugol’s) potassium iodide iodone
Inorganic Iodines MOA: acutely blocks release of thyroid hormone from the gland by inhibiting thyroglobulin proteolysis inhibit iodide organification Uses: useful in thyroid storms: 2-7 days Preoperatively - iodides decrease vascularity, size and fragility of hyperplastic gland Caution: it may delay onset of thioamide effects; should be given after initiation of thioamides The gland will escape from inhibition after 2-8 weeks.
Iodinated Contrast Media Iodinated contrast media Ipodate (oral) Iopanoic acid (oral) Diatrizoate (intravenous) valuable in hyperthyroidism (but is not labeled for this indication) MOA: inhibits conversion of T4 to T3 in the liver, kidney, brain and pituitary Another MOA is due to inhibition of hormone release secondary to iodide levels in blood Useful in thyroid storms (adjunctive therapy)
Beta Blockers Drugs: Propranolol, Metoprolol, Atenolol MOA: Membrane-stabilizing action: inhibits T4 to T3 Ameliorate many disturbing s/sxs of hyperthyroidism secondary to increased circulating catecholamines by blocking beta receptors Indications: Grave’s, Thyroid storm
Corticosteroids Prednisone is given for patients with Grave’s ophthalmopathy 1mg/kg/day (60mg/day 3 divided doses); if it should be given for more than 4 weeks, taper to decrease risk of adrenal crisis
Thyroid storm • Sudden exacerbation of throtoxic symptoms • Life threatening condition • Vigorous management • Propanalol 1-2mg i/v or 40-80mg PO Q6h • Diltiazem 90-120mg Po Q8-6 hrs or 5-10mgs intravenous infusion/hour
Thyroid storm • Potassium iodide • Propylthiouracil • Hydrocortisone • Supportive therapy • Plasmapheresis/peritoneal dialysis
Hyperthyroidism and Pregnancy • Ideal situation- treat before pregnancy • Pregnancy-Radioactive iodine CI • Propylthiouracil • Dose limitation≤ 300mgs/day • Methimazole alternative- fetal scalp defects