Download
1 / 31
320 likes | 564 Views
Pulse Oximetry screening for Cardiac malformations in the neonate. Majd Abu-Harb. September 2014. Congenital Cardiac malformations. 6-10% of all infant deaths 74% of all CCM are diagnosed in infancy and most of these present during the neonatal period

E N D
Pulse Oximetry screening for Cardiac malformations in the neonate Majd Abu-Harb September 2014
Congenital Cardiac malformations • 6-10% of all infant deaths • 74% of all CCM are diagnosed in infancy and most of these present during the neonatal period • 96% of those who survived infancy will go on to survive into adulthood
Congenital Cardiac malformations • Many babies are asymptomatic at birth • More than 50% babies with CM may be missed by neonatal exam* • Earlier discharge reduces time-window for signs and symptoms to develop * Wren et al. Arch Dis Child Fetal Neonatal Ed 1999;80:F49-F53
Modes of presentation in the neonate • Left heart obstruction • Right heart obstruction • Abnormal connections
Modes of presentation • Left heart obstruction • Right heart obstruction • Abnormal connections Heart failure
Modes of presentation • Left heart obstruction • Right heart obstruction • Abnormal connections Heart Failure Cyanosis
Heart Failure • Left heart obstruction Coarctation of the Aorta
Right heart obstructive lesions Diminished pulmonary blood flow Cyanosis
Abnormal connections Problem with mixing Cyanosis Transposition of the great arteries
Newborn screening NN check: murmur abnormal pulses
Our audit of early neonatal murmurs(2008-9) • All babies born in Sunderland undergo new born check in hospital even if delivered at home • All babies with murmurs can be evaluated prior to discharge
Retrospective - hospital based All births over 2 year Total births 6874 Exclusions: prenatal diagnosis preterm < 35 wks symptomatic prior to NN examination admissions to NICU 6560 included in the analysis
Of 6560 babies 70 had murmurs (Prevalence 1%) Age of baby when murmur was detected 12-36hrs Hospital stay: range 10-96 hrs ( mode 21.5hrs) Of those with murmurs 23 had structural CM ( 33%) Our audit
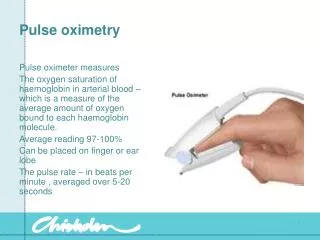
Screening • Antenatal : Anomaly scan detection rate variable • NN check • Pulse oximetry: - Clinically undetectable low oxygen levels present in the majority of critical CM - Pulse oximetry may detect babies with Critical CM early, before they collapse
Measurement of oxygen saturation once in one foot of all babies after 2 hrs and before discharge
The oxygen saturation study • All babies whose oxygen saturation below 95% had echocardiography • 2 year birth cohort based at Sunderland April 1999-March 2001 • Total live births: 6166 • 5719 babies eligible for measurement • 5626 (98.3%) measured
Oxygen saturation study Babies with Sat. measured 5625 Total births 6166 296 Sat. low ( 49 ) CHD ( 10 ) CHD ( 12 ) Other significant pathology
Babies with Sat. measured 5625 Oxygen saturation study 296 Sat. low ( 12 ) Other 10 Respiratory 2 CNS ( 10 ) CHD 3 No murmur 7 Murmur 1 Coarctation 2 Transposition
Critical Cardiac malformations • ~ 1.7/1000 live births • Estimated 1200 new cases per year in England and Wales • May only be recognised when babies collapse • Hypoplastic Left heart Syndrome (HLHS) • Pulomanry atresia with Intact ventricular septum (PA /IVS) • Interrupted Aortic Arch (IAA) • Transposition of the Great Arteries (TGA) • Those dying or undergoing operation/intervention before 12 weeks of age with the following • PA with VSD • Coarctaion of the aorta (CoA) • Aortic stenosis (AS) • Total anomalous pulmonary venous connection (TAPVC)
2007 -Systematic review ; 8 studies 35 950 patients Thangaratinamet al . Arch Dis Child Fetal Neonatal Ed 2007,92:F176-F180 “More Larger studies needed to define test accuracy” 2011 PulseOx: a test accuracy study Ewer et al . The Lancet, Volume 378, Issue 9793, pages 785-794, 27 August 2011 20 055 babies screened ( of which 24 cases had Critical CM) Test positive -18/24 critical cases - 14 non-critical CM Accuracy for Critical CM : sensitivity 75% vs 50% antenatal us False negatives : 6 Critical CM ( 4 of which detected on AN screen ) False positives: 169 (0.8%) of these 6 had significant CM, 40 had other conditions including pneumonia Oximetry studies
2013 -Neonatal screening for critical CM using pulse oximetry Prudhoe et al Arch Dis Child Fetal Neonatal Ed 2013;98:F346-F350 13 previous studies listed –published birth cohorts 1998-2009 Single centre study (1999-2009) 29 925 babies screened ( of which 27 had Critical CM) Test positive - 5/27 critical cases - 5/50 serious cases “Routine pulse oximetry did not prevent five babies with critical and 15 with serious anomalies being discharged undiagnosed. Results from screening over 250 000 babies have now been published, but this total includes only 49 babies with transposition, and even smaller number of rarer anomalies” 3 more studies have been published since ….. Oximetry studies
What do have oximetry screening (OS) studies in common? • OS is effective in significant hypoxaemia i.e. most obstructive right heart lesions • OS is not good at detecting Coarctation of the aorta • The advantage of detecting non-cardiac serious illnesses
Practical issues • Antenatal detection rate of CM • False positive rate and impact on: - admission - workload - parental anxiety • Timing of screening • Acceptability and cost-effectiveness • Wider implementation of OS in the UK?
Birmingham Women’s Hospital data • 40 month period • Live births : 25859 • Total admissions 3552 of which 1651 were unexpected - 208/1651 (12.6%) for test +ve OS - Echo was performed in 61/208 - 165/208 had significant clinical condition 17 CM ( 9 critical) 55 pneumonia 30 sepsis 12 PPHN Therefore 1/8 of the unexpected admissions was due to positive OS but less than third of these had echo performed Singh A et al . Arch Dis Child Fetal Neonatal Ed 2014;99:F297-F302
ConclusionsRoutine pulse oximetry screening: • is feasible and acceptable to parents and staff • adds value to existing screening procedures • is likely to identify cases of Critical CM which would otherwise go undetected • has the additional advantage of detecting other serious ( non-cardiac ) illnesses