Download
1 / 69
690 likes | 846 Views
Impact of New Anticoagulants on the Blood Bank. January 24 th , 2012 Transfusion Medicine Resident Teaching Session Dr. Sudeep Shivakumar, Hematology. Objectives. To briefly review the concepts of hemostasis and thrombosis To provide an overview of anticoagulants currently in use

E N D
Impact of New Anticoagulants on the Blood Bank January 24th, 2012 Transfusion Medicine Resident Teaching Session Dr. Sudeep Shivakumar, Hematology
Objectives • To briefly review the concepts of hemostasis and thrombosis • To provide an overview of anticoagulants currently in use • To discuss the new anticoagulant agents and their mechanism of action • To review the evidence for the new anticoagulants in DVT/PE and atrial fibrillation • To discuss implications of these medications for the blood bank
Overview • Anticoagulants are widely used • Vitamin K antagonists used to be the only oral option • Times are changing…
Overview • Big advantage: • No lab monitoring • Big disadvantage: • No lab monitoring • Unpredictability of coagulation tests • No reversal agents • Variety of different agents with different characteristics
Background • What are anticoagulants? • Substances that prevent blood from clotting • “Blood thinners” • How do they do this? • Interfering with coagulation mechanisms
Hemostasis • Complex process which causes bleeding to stop: • Formation of blood clot formation at the site of vessel injury • Carefully regulated system • Involves platelets and coagulation factors • Lack of coagulation factors bleeding • Overactive coagulation cascade thrombosis
Thrombosis • The formation of a blood clot within a blood vessel • Can occur in the arterial or venous systems • Leads to obstruction of a blood vessel in the circulatory system • Can lead to ischemia and infarction, and even death • Can also lead to embolism • Clot within a vessel breaks free and travels through body (“embolizes”) • Thromboembolism is combination of a thrombosis and embolus
Atrial fibrillation • Most common cardiac rhythm disorder • Affects >10% in those > 80 years old Incidence of atrial fibrillation in 4000 male air crew recruits Krahn et al, Am J Med, 1995
Atrial fibrillation • Lifetime risk for a 40 year old is ~25% (Framingham1) • Independent risk factor for ischemic stroke • Rate of stroke in those not on antithrombotic therapy is ~4.5%/year • Increases the risk of stroke 5x across all age groups • Incidence of stroke increases with age2 • 1.3% per year for those aged 50-59 • 5.1% per year for those aged 80-89 1Wolf, Stroke, 1991 2Frost, Am J Med, 2000
Anticoagulants in atrial fibrillation • Goal is to prevent stroke • Reduces risk to ~1% per year • Warfarin shown to be more effective than aspirin
Warfarin in atrial fibrillation Warfarin Better Control Better AFASAK SPAF BAATAF CAFA SPINAF EAFT Aggregate -100% 50% -50% 100% 0 Hart R, et al. Ann Intern Med 1999;131:492
Anticoagulants in atrial fibrillation • Most recent Canadian Cardiovascular Society guidelines (2010): • Patients with CHADS2 score of 1 or higher should be on oral anticoagulants
Venous thromboembolism Deep venous thrombosis Pulmonary embolism
Venous thromboembolism • Venous stasis Hypercoagulability Vessel wall injury Incidence estimated at 1-2 in 1000 Known predisposing conditions – Virchow’s triad:
Venous thromboembolism • Not uncommon • Longitudinal investigation of thromboembolism etiology (LITE) study1 • >21 000 participants • Cohort study • Incidence of 1st time VTE = 1.92 per 1000 person years • Major cause of morbidity and mortality • JAMA study2 looking at post-mortems of 3 412 hospitalized patients between 1966 and 1980 • 6% of deceased patients had evidence of massive pulmonary embolism • Most common preventable cause of in-hospital death 1Cushman, Am J Med, 2004 2Dismuke, JAMA, 1986
Pulmonary embolism • Untreated PE • Mortality rate of ~30%1 • Most die within hours of diagnosis • Treated PE • Prospective NEJM study looked at 399 patients with newly diagnosed PE • 94% received anticoagulant treatment • Only 2.5% (10 patients) died of PE • Treatment of PE is life-saving! 1Dalen, Prog Cardiovasc Dis, 1975 2Carson,NEJM, 1992
Anticoagulants in DVT/PE • Goals of treatment: • Short term: • Prevent the extension of thrombus and embolization for DVT • Reduce mortality for PE by reducing recurrent events • Relief of symptoms • Long term: • Prevent recurrent events
Anticoagulants currently used • Unfractionated heparin • Low molecular weight heparin • Vitamin K antagonists • Ie. warfarin
Warfarin • Can be reversed: • Vitamin K • Fresh frozen plasma • Activated prothrombin complex concentrates
Warfarin • Dosage varies because of: • Vitamin K status • Dietary factors • Nausea/vomiting • Absorption • Activity level • Other medications • Genetics • Monitoring by INR necessary!
Difficulties with warfarin use • Requires monitoring • Numerous drug and diet interactions • Narrow therapeutic range • Difficult to control – takes time to get in or out of the system Role for new anticoagulants?
New anticoagulants • Many new targets being explored • Eg. thrombin, factor Xa, tissue factor, protein C, factor V and VIII • New agents developed • Direct thrombin inhibitors • Factor Xa inhibitors • Novel anticoagulants • Oral agents increasingly in studies • Venous thromboembolism often studied first because of shorter follow up • Increasing data on dabigatran and rivaroxaban
New anticoagulants • Ideal anticoagulant: • Equally efficacious • Equally safe • No monitoring • Fewer interactions • Oral • Reversible
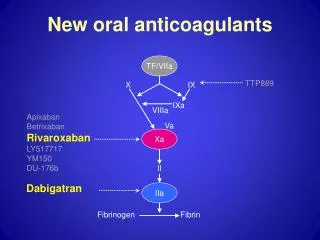
New anticoagulants • Direct thrombin inhibitors • Dabigatran • Factor Xa inhibitors • Rivaroxaban
New anticoagulants Leung, The Hematologist, 2011
Dabigatran • Ximelagatran studies showed possible use for oral direct thrombin inhibitors in atrial fibrillation • Dabigatran • Oral prodrug of dabigatran etixalate • Inhibitor of thrombin • Predictable anticoagulant response • No need for monitoring • Excreted by kidneys • Less than 1% see a transaminase elevation
Dabigatran • An ideal anticoagulant: • No monitoring • Fewer interactions • Oral • Reversible • Equally efficacious • Equally safe
Dabigatran ✓ ✓ ✓ ✗ ? ? • An ideal anticoagulant: • No monitoring • Fewer interactions • Oral • Reversible • Equally efficacious • Equally safe
Dabigatran • Pharmacokinetics • Half life 12-17 hours • Time to peak, plasma 1 hour • Hepatic metabolism • Not recommended for CrCl <30
Dabigatran • Many studies for VTE prophylaxis: • REMODEL – thromboprophylaxis after knee surgery • REMOBILIZE – thromboprohylaxis after knee surgery • RENOVATE I and II – thromboprophylaxis after hip surgery • Studies for VTE treatment: • RECOVER – acute VTE treatment • REMEDY – secondary VTE prevention • Studies for atrial fibrillation: • PETRO study – phase II • RELY study – phase III
Dabigatran for atrial fibrillation • RELY trial • Looked at stroke prevention in patients with atrial fibrillation • Compared warfarin to dabigatran • >18 000 patients • Results: • 110 mg BID dose of dabigatran as effective and less bleeding • 150 mg BID dose more effective, similar bleeding • Published in NEJM in September 2009 (Connolly et al)
Dabigatran for atrial fibrillation • RELY trial • Note trend towards increased MI rates with dabigatran 150 mg BID • Also increased dyspepsia • Consider higher dose if <80 and low risk of bleeding
Dabigatran for VTE • RECOVER trial • Dabigatran exilate vs warfarin in the treatment of acute thromboembolism • Randomized double blind trial • 2539 patients with acute VTE • All treated initially with 5 to 11 days of LMWH or UFH • Randomized to dabigatran 150 mg BID vs warfarin • Primary outcome: objective recurrent VTE, or VTE-related death up to 6 months of treatment
Dabigatran for VTE • RECOVER trial • Results: • Recurrent VTE: • 34 patients (2.7%) in dabigatran group • 32 patients (2.5%) in warfarin group (not significant) • Major bleeding: • 20 patients (1.6%) in dabigatran group • 24 patients (1.9%) in warfarin group (significant) • Deaths similar between groups • Conclusions: • Dabigatran as safe and efficacious as warfarin • Published in NEJM in December 2009 (Schulman et al)
Dabigatran • Approved by Health Canada for atrial fibrillation • Not covered by MSI… yet • Not approved for VTE treatment • Costs $2.30 per day
Dabigatran and coagulation assays • aPTT affected at peak concentrations • aPTT >90 sec suggests over-dosing or accumulation • PT not affected • Fibrinogen testing underestimated results in 2 of 4 reagents • Antithrombin levels varied greatly • Overall, unpredictable results, but elevated aPTT suggested accumulation
Factor Xa inhibitors • Lack of direct thrombin inhibition = less bleeding?
Rivaroxaban • Oral, direct factor Xa inhibitor • Potent (greater selectivity for factor Xa than other drugs) • Fixed, once-daily dosing • Predictable pharmacokinetics • Half life 7-11 hours • Peak concentration 4hrs after administration • Excreted via biliary and renal routes • Does have interactions CYP3A4 inhibitors • Ie. ketoconazole, macrolides