Download
1 / 85
850 likes | 860 Views
This training program, offered by the Arkansas Department of Health, provides school nurses with the knowledge and skills to prevent and address obesity in children. It covers topics such as defining obesity, discussing risk factors, health consequences, and legislation related to BMI. Resources available for schools and school nurses to combat childhood obesity are also highlighted.

E N D
Obesity Prevention Education and Body Mass Index (BMI) Training for School Nurses
Arkansas Department of Health is an approved provider of continuing nursing education by Midwest Accreditation Program, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation
The planning committee & faculty attest that no relevant financial, professional or personal conflict of interest exists, nor was sponsorship of commercial support obtained, in the preparation or presentation of this educational activity.
Objectives • Define obesity and relate current trends in Arkansas and in the US. • Discuss risk factors for childhood obesity. • Explain health consequences of obesity. • Review history and pertinent legislation related to BMI in Arkansas • Demonstrate the process for appropriate height and weight measurement for children. • List resources available for schools and school nurses to combat childhood obesity.
Definition of Obesity Obesity is defined as an increased body weight in relation to height, when compared to some standard of acceptable or desirable weight.
Obesity and Overweight in Children Obesity in children and youth refers to age and gender- specific BMI that is equal to or greater than the 95th percentile of the CDC BMI charts Overweight/at risk for obesity in children and youth refers to a BMI that is between the 85th – 94th percentile (IOM, 2007)
In the Past Three Decades… Number of overweight: • 6-11 year olds tripled • Adolescents tripled • Overweight adults tripled
The Epidemic of Obesity • Obesity affects 17% of all children and adolescents -12.5 million children and adolescents • More than 1/3 of adults are obese www.cdc.gov
Obesity in the United States http://www.cdc.gov/obesity/data/trends.html
DietInactivity High-calorie foods High-fat foods dense in calories Soft drinks, candy, and desserts high in sugar/calories Sedentary kids more likely to gain weight Inactive leisure activities
Genetics Overweight family and child may be genetically predisposed to put on excess weight environment of high-calorie foods physical activity may not be encouraged
Heredity and Genes 80%of children with two overweight parents will become overweight 40%of children with one overweight parent will become overweight 7–9%of children with no overweight parents will become overweight http://www.surgeongeneral.gov/topics/obesity/calltoaction/fact_adolescents.htm
Some eat to cope with problems or deal with emotions; stress or boredom Parents may have similar tendencies Psychological
Environmental and Media: Temptation at Every Turn Chips, cookies, cereal, fast food, and other less healthy food choices are marketed to children via media
Behavioral and Socio-cultural Sedentary lifestyles Calorie-dense foods Large portion sizes Excessive screen time low energy expenditure Parent modeling - eating and exercise behaviors
Risk of CVD Hypertension Elevated insulin levels Dyslipidemia Elevated low density lipoprotein (LDL) Abnormal triglyceride levels
Psychosocial • Quality of Life • Depression and Anxiety • Negative self-esteem and poor body image • Feelings of chronic rejection, withdrawal from interaction with peers, and behavioral problems • Decreased endurance and/or participation • Social, academic and discrimination (bullying/teasing) www.cdc.gov
Other Health Consequences • Sleep apnea • Asthma • Risk for Kidney problem • Orthopedic disorders • Skin fungal infections • Gastrointestinal • fatty liver disease • elevated liver enzymes • gallstones and cholecystitis • gastroesophageal reflux • constipation
Other Health Consequences Cancer • Esophageal • Breast • Endometrial • Colon/rectal • Kidney • Gall Bladder • Thyroid • Pancreas
Other Health Consequences • Endocrine disorders • T2DM • Acanthosis Nigricans • Polycystic Ovary Syndrome • Early sexual maturation Clearly, the growth in the treatment of type 2 diabetes could signal the beginning of a multitude of long-term healthcare needs for many of these children
Acanthosis nigricans type III associated with obesity, insulin-resistant states and endocrinopathy Acanthosis nigricans is a disorder that may begin at any age Velvety thickening Gray to brown to black in body creases Neck, armpits, groin Darker skinned people have darker lesions http://www.aocd.org/skin/dermatologic_diseases/acanthosis_nigrica.html (James, et al 2005)
Economic Burden of Obesity The Economic Estimates of the impact of obesity are astronomical: 1995 - Approximately $52 billion was attributed to obesity 2006 - This figure had increased to $147 billion Researchers have estimated that by 2030, if obesity trends continue unchecked, obesity-related medical costs alone could rise by $48 to $66 billion a year in the U.S.
Economic Burden of Obesity Obesity is the No. 1 driver of increasing health care costs in the US today Diabetes contributes to health care disparities in the United States
Rising obesity rates - result of a number of trends in the US (F as in Fat, 2009) Nutritious foods are more expensive than calorie-dense, less nutritious foods Americans walk less and drive more -- even for trips of less than one mile Adults often work longer hours & commute farther (convenience food) Parks & recreational spaces are not considered safe or well maintained in many communities Children engage in less physical activity in school ↑ screen time
AR Preventive Nutrition and Physical Activity Summit • Purpose: to develop specific strategies to control the obesity epidemic in Arkansas • Occurred: March 8, 2003 • Funded by: National Institute of Health Nutrition Academic Award • Support from: UAMS, ADH, ACHI, ACH, others • State-wide summit
Act 1220 of 2003 • Creates an Arkansas Child Health Advisory Committee • Limits access to food/beverage vending machines • Reports ALL money received from food and beverage contracts. • Convenes an advisory committee in each school district • Incorporates nutrition/physical activity goals into annual plans
Act 1220 of 2003 States: “Require schools to include as part of the Student Health report to parents an annual body mass index percentile by age for each student; and require schools to annually provide parents with an explanation of the possible health effects of body mass index, nutrition, and physical activity.” (in a confidential, private and accurate manner)
Act 201 of 2007 • Individual students will participate in BMI assessments in kindergarten and in grades 2, 4, 6, 8, and 10. • BMI measurements will be eliminated for students in grades 11 and 12.
Act 201 of 2007 • Parents can provide written notice to the school if they choose to exclude their children from BMI assessments. • Community Health Nurses will work with schools to assure that proper protocol is followed during the BMI assessments.
UAMS College of Public Health Evaluation of Act 1220: Year 7 • Parents are maintaining their awareness of short- and long-term health problems associated with childhood obesity • 90% of parents said that obesity is a serious problem for the state • 79% of parents indicated that they believe schools play an important role in combating childhood obesity
UAMS College of Public Health Evaluation of Act 1220: Year 7 • The percentage of parents preferring that students take PE 3 or more times per week has increased since 2009 • Schools are more frequently offering nutritional information for students. • No significant evidence of a negative impact on students
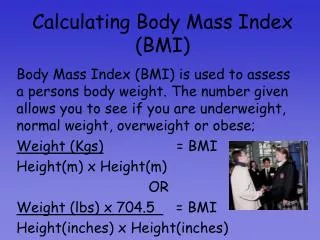
AAP Recommendation Accurately weigh and measure to monitor growth Calculate and plot BMI once a year in all children and adolescents Use changes in BMI to identify rate of excessive weight gain relative to linear growth (AAP, 2003, reaffirmed in 2007)
Childhood BMI is gender & agespecific (CDC, 2009) http://www.cdc.gov/nccdphp/dnpa/obesity/childhood/defining.htm
BMI for Age and Gender: Used for children and teens because of their rate of growth and development Provides a reference for adolescents that can track body size throughout life Compares well to laboratory measures of body fat (Barlow, 2007)
Body Mass Index What it is and is not! An inexpensive, effective, easy-to-perform screening tool using height and weight -Not intended to be used as the sole diagnostic measure (CDC)
Perspectives About the Use of BMI Measurement Identify referrals and resources for children and parents Promote policies that access to healthful foods and daily physical activity
Prior to Assessment • Contact school administration and teachers • Determine assessment team • Screener • Recorder • Determine date and place and which students to be assessed
Day of Assessment • Equipment • Calibration of scales • Station set up • Preparation of child • Data collection forms or computer
Recommended Equipment • Stadiometer (page 4 in training manual) • Measures height • Portable or permanently affixed to wall • Provided by ACHI • Tape wood board to wall for stability • Carpenter’s triangle for headpiece
Scales • Tanita HD-314 • Portable • Measures up to 330 lbs • Digital read-out • Tanita HD-351 • Portable • Measure up to 440 lbs • Digital read-out • Previous weight is visible
Recommended Equipment Step Stool -Height measurements to ensure measurement line is read at eye level Batteries (Check type & number required) Name Tags – children and staff Office Supplies Container for personal items