Download
1 / 43
430 likes | 445 Views
This study examines the effects of different ß-blocking agents in reducing mortality in congestive heart failure, with a focus on carvedilol, metoprolol, and bisoprolol. The findings show that carvedilol has the greatest mortality reduction effect compared to other ß-blockers.

E N D
Results of the Longest and Largest Everb-Blockade Study in CHFMortality Reduction beyond ß1-Blockade Pub.: Results: Poole-Wilson et al. Lancet 2003;362:7-13 Design: Poole-Wilson et al. Eur J Heart Fail 2002;4:321-329
Pharmacological Differences Within the b Blocker ClassAgents currently evaluated for heart failure b1b2a1Ancillary blockadeblockadeblockade ISA effects* Carvedilol +++ +++ +++ - +++ Metoprolol +++ - - - - Bisoprolol +++ - - - - Bucindolol +++ +++ -++ - *anti-oxidant, anti-endothelin, anti-proliferative lack of b1receptor upregulation
b1 b1 b1 b1 b1 b1 b1 b1 b1 b1 b1 b2 b2 The Normal Heart is a b1-Organ thatFunctions in a b1-Environment Normal
b2 b1 b1 b2 b1 b1 b1 a1 b1 b1 b1 b1 b1 b1 b1 b1 b1 b2 b2 a1 b2 b1 b1 b1 b1 b1 b2 b2 b2 Heart Failure Converts the Circulation From a b1 to a b1/b2/a1-Environment Normal Heart failure
Effects of 2-Receptors • Direct chronotropic, inotropic, lusitropic cAMP mediated • Coupling to the GS/cAMP pathway greater than via 1-adrenoceptor, further enhanced by selective 1-blockade • Newton et al. Circ 1999; Kaumann et al. Circ 1999 • Hall et al. Circ Res 1990 • Hypertrophy, fibrosis, remodelling • Du et al. Circulation 2000 • Antiapoptotic • Communal et al. Circulation 1999 • Arrhythmogenic • Billman et al. Circulation 1997 • Facilitation of norepinephrine release (presynaptic) • Boudreau et al. Am J Physiol 1993
Effects of 1 Receptors • Myocardial hypertrophy, fibrosis, remodeling • Simpson & McGrath, J Clin Invest 1983 • Morgan & Baker, Circulation 1991 • Cardiotoxicity (with receptors) • Mann et al. Circulation 1992 • Arrhythmogenic • Molina-Viamonte et al. Circulation 1991 • Peripheral vasoconstriction • Leier et al. Circulation 1990 • Renal hypoperfusion and sodium retention • Smyth et al. Circ Res 1985 • Hesse et al. Br J Pharmacol 1985
Bisoprolol Metoprolol Effects of Different b Blocking Agents Pharmacological differences Sympathetic activation 1 receptors 2 receptors 1 receptors Carvedilol Cardiotoxicity
Carvedilol, But Not Metoprolol, Reduces Total Body and Cardiac Sympathetic Drive Total BodyNorepinephrine Spillover CardiacNorepinephrine Spillover 100 0.5 50 0 0 -0.5 (nmol/min) (nmol/min) -50 -1.5 -100 * * -150 -2.5 Carvedilol Metoprolol Carvedilol Metoprolol Azevedo et al. Circulation 2001 * P < 0.05 vs. baseline and vs. metoprolol
0 0.2 0.4 0.6 0.8 1 Mortality Results of Blockers Studies in CHF Trial n Hazard Ratio (95% CI) MERIT-HF 3,991 0.66 (0.53-0.81) US Carvedilol Prog 1,094 0.35 (0.20-0.61) CIBIS II 2,647 0.66 (0.54-0.81) BEST 2,708 0.90 (0.78-1.02) COPERNICUS 2,289 0.65 (0.52-0.81) Mild to Moderate Severe Packer et al. NEJM 1996; CIBIS II Invest. Lancet 1999; MERIT-HF Study Gp. Lancet 1999 BEST Investigators. Lancet 1999; Packer et al. NEJM 2001
COPERNICUS US Carvedilol Programme Survival Survival 1.0 0.9 0.8 0.7 0.6 0.5 Carvedilol 100 90 Carvedilol Placebo 80 Placebo 70 Risk reduction = 65% Risk reduction = 35% p=0.00013 p<0.001 60 0 0 50 100 150 200 250 300 350 400 0 3 6 9 12 15 18 21 Days Months Packer et al (2001) Packer et al (1996) Survival Mortality (%) 1.0 CIBIS-II MERIT-HF 20 Placebo Bisoprolol 15 0.8 Metoprolol CR/XL 10 Placebo Risk reduction = 34% Risk reduction = 34% 0.6 5 p=0.0062 p<0.0001 0 0 0 200 400 600 800 0 3 6 9 12 15 18 21 Time after inclusion (days) Months of follow-up The MERIT-HF Study Group (1999) CIBIS-II Investigators (1999)
Herzinsuffizienz: NNT* - Number Needed to Treat for one year to save one life NYHA II-III NYHA II-III NYHA IV NYHA (II-) III *NNT= Wie viele Patienten muss man 1 Jahr lang behandeln, um einen Todesfall zu verhindern? Die NNT basiert auf der absoluten Mortalitätsreduktion gegenüber Placebo über eine Zeitperiode von genau 1 Jahr, nach Wehling M., J Kardiol 2003;10 (Suppl A) p 20-23
Metaanalyse Betablockade bei Herzinsuffizienz: Verbesserung der Herzleistung P=0,009 P=0,0002 Veränderung der LV-Auswurffraktion als Marker für die Herzfunktion unter der Therapie mit Carvedilol bzw. Metoprolol. Daten aus einer Metaanalyse von 4 direkten Vergleichsstudien bzw. 15 Placebo-kontrollierten Studien (Veränderung gegen Placebo) zwischen Carvedilol und Metoprolol Nach M. Packer, Am Heart J 2001; 141:899-907
Metoprolol Carvedilol Carvedilol Improves Cardiac Performance to a Greater Extent than Metoprolol LV Ejection Fraction LV EDV LV ESV 0 16 P = 0.038 -5 14 *** -10 12 -15 10 *** Absolute change from baseline ml/m2 LVEF (%) -20 8 ** -25 6 *** -30 4 *** 2 -35 *** 0 -40 **P < 0.01 ***P < 0.001vs baseline Metra M et al. Circ 2000
Meta-analysis of Direct Comparison Trials with Metoprolol and Carvedilol in CHF +12 P = 0.009 +10 +8 LV Ejection Fraction (%) +6 +4 +2 0 Metoprolol (n = 123) Carvedilol (n = 125) Packer M et al. Am Heart J 2001
Blocker Tolerability in Clinical Trials Percentage of patients achieving target dose Bisoprolol (CIBIS II) Metoprolol (MERIT-HF) Carvedilol (US Carvedilol) Carvedilol (COPERNICUS) 0 20 40 60 80 100 %
COMET: Objectives and Design • To compare the effects of the combined alpha/betablocker carvedilol with those of the ß1-selective metoprolol on mortality and morbidity in patients with chronic heart failure • No run-in period Randomisation Carvedilol (n = 1,511) Mild, moderate or severe CHF Metoprolol (n = 1,518) Screening Titration Maintenance (estimated 4 - 6 yrs)
COMET Trial • The COMET trial is not simply a comparison of the survival effects of Metoprolol and Carvedilol in patients with heart failure. • The COMET trial is really a test of whether the properties of Carvedilol beyond 1-blockade have favorable effects on survival. • To verify this theory, Metoprolol and Carvedilol were used in dosages, that produce equivalent degrees of 1-blockade (50 mg Metoprolol IR BID and 25 mg Carvedilol BID)
Dates, Timing and Follow-up First patient recruited: Last patient recruited: Total recruited: Carvedilol: Metoprolol: 01-Dec-1996 15-Jan-1999 3029 1511 1518 Minimum follow-up (months): Maximum follow-up (months): Average follow-up (months): 47 71 57.9 Total patient months of follow-up: Total deaths prior to 15-Nov-2002: 175447 (=14621 years) 1112
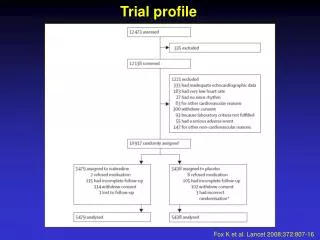
Flow Chart of Patients Randomised 3029 Carvedilol 1511 Metoprolol 1518 Assigned to drug and received at least one tablet Withdrew consent 10 Lost to follow-up 3 Withdrew consent 18 Lost to follow-up 2
Main Inclusion Criteria • Symptomatic CHF (NYHA II-IV) on standard treatment • Stable diuretic treatment 2 weeks • ACE inhibitor 4 weeks prior to study entry • use of digitalis and/or vasodilators was discretionary • LVEF 35% • 1 CVS hospitalisation in the previous 2 years
Severity of Heart Failure COMET MERIT-HF1 N=3,029 N=3,991 NYHA Class (%)II 48 41III 48 55IV 4 4 LVEF (%) 26 28 1. Lancet 1999; 353: 2001-7
Background Therapy COMET MERIT-HF Diuretic 99% 90% ACEi 91% 90% ARB 7% 7% Spironolactone 11% 8% Digoxin 59% 64% Aspirin 37% 46% Warfarin 46% NA
COMET: Baseline Characteristics Carvedilol (n=1511) Metoprolol (n=1518) Age (y, mean/sd) 61.6 (11.3) 62.3 (11.4) Male (%) 79.4 80.2 Aetiology (IHD %) 52 54 Months of HF (mean/median) 42.6/22 42.2/20 Heart rate (beats/min) 81 81 Systolic BP (mm Hg) 126 126 Diastolic BP (mm Hg) 77 77 NYHA class (%) II/III/IV 48/48/3 49/47/4 AF/flutter (%) 20.5 19.2 Diabetes 23.8 24.4
COMET: Primary Endpoint Total Mortality 40 Metoprolol 30 20 Carvedilol Mortality (%) Hazard ratio 0.83, 95% CI 0.74 – 0.93, P = 0.0017 10 0 0 1 2 3 4 5 Time (years) Number at risk Carvedilol 1511 1367 1259 1155 1002 383 Metoprolol 1518 1359 1234 1105 933 352 Poole-Wilson et al. Lancet 2003;362:7-13
40 Metoprolol 30 Mortality (%) 20 Carvedilol 10 Survival benefit 20%, P = 0.0004 0 0 1 2 3 4 5 COMET: Cardiovascular Mortality Time (years) Number at risk Metoprolol Carvedilol 1,518 1,359 1,234 1,105 933 352 1,511 1,366 1,258 1,155 1,002 383 ESC 2003
Event % 15 Metoprolol Carvedilol 10 5 0 1 2 3 4 5 COMET: Fatal or non-fatal myocardial infarction Hazard ratio 0.714 95% CI 0.523 - 0.974, p=0.0333 - 29% Time (years) K. Swedberg AHF 2003, Las Vegas
COMET-Studie: Unterschiede in der Mortalität Carvedilol versus Metoprolol -17% -20% P=0,0017 P=0,0004 Poole-Wilson P. et al. Lancer 2003; 362:7-13
COMET: Risikoreduktion gegenüber kardioselektiven Betablocker Metoprolol p=0,0017 p=0,0004 p=0,0333 Nach P. Poole-Wilson, ESC 2003, Wien und K. Swedberg AHF 2003, Las Vegas
COMET: Mode of Death Carvedilol Metoprolol n=1511 n=1518 Sudden 218 (42.6%) 262 (43.7%) Circulatory failure 168 (32.8%) 197 (32.9%) Stroke 13 (2.5%) 38 (6.3%) Other CV 19 (3.7%) 26 (4.3%) Non-CV 74 (14.5%) 66 (11.0%) Unable to classify 20 (3.9%) 11 (1.8%)
COMET: Death from Stroke Relative Risk Reduction 67% !! P = 0.0006 3 Metoprolol 2 Carvedilol Mortality (%) 1 0 0 1 2 3 4 5 Time (years) ESC 2003
COMET: Consistent Mortality Reduction in Sub-Groups Male (n = 2.417) Sex Female (n = 612!) Age < 65 65 NYHA II III IV (n = 115!) Cause Other IHD LVEF 25% > 25% Heart rate < 80 80 Systolic BP < 110 110 - 139 140 Diabetes yes no Overall Metoprolol better Carvedilol better 0.50 0.75 1.00 1.25 1.50 Poole-Wilson et al. Lancet 2003;362:7-13
COMET: Secondary Endpoints Secondary endpoints Carvedilol Metoprolol Hazard ratio 95% CI P-value Death and cardiovascular hospitalisation 963/1511 63.7% 1016/1518 66.9% 0.928 0.85, 1.014 0.0972 Cardiovascular death, heart transplantation or hospitalisation for non-fatal AMI or worsening heart failure 745/1511 49.3% 815/1518 53.7% 0.881 0.798, 0.974 0.0128 Death and hospitalisation for worsening heart failure 774/1511 51.2% 841/1518 55.4% 0.89 0.807, 0.981 0.0191
COMET: New Onset Diabetes Relative Risk Reduction 22%, P = 0.04 15 10 Metoprolol New diabetes (%) 5 Carvedilol 0 0 1 2 3 4 5 Time (years) Number at risk Metoprolol 1,147 991 879 764 626 221 Carvedilol 1,151 1,014 908 827 705 254 ESC 2003
COMET – ESC, Wien 2003: Risikoreduktion Carvedilol im Vergleich zu Metoprolol P=0,04 P=0,006 Poole-Wilson P. ESC-Wien, 2.9.03
COMET: Events Related to b Blockade Carvedilol Metoprolol n = 1511 n = 1518 Bradycardia as AE 9.5% 8.9% Bradycardia as SAE 2.6% 2.6% Hypotension as AE 14.2% 10.5% Hypotension as SAE 3.2% 1.9%
Summary • The COMET trial compared dosing regimens of metoprolol and carvedilol that produced similar degrees of 1-blockade, both at peak and at trough • The results of the COMET trial indicate that the actions of carvedilol beyond 1-blockade have favorable effects on survival
Summary and conclusion • First head-to-head mortality study comparing two beta-blocking agents in CHF • Carvedilol saved significantly more lives than metoprolol (by 17%, P = 0.0017) and reduced cardiovascular mortality by 20%, p=0,0004 • Carvedilol compared to metoprolol reduced annual mortality from 10.0% to 8.3% and prolonged median survival by 1.4 years • Carvedilol is the preferred beta-blocker for the treatment of chronic heart failure
Betablockade: Mortalitätsreduktion bei HI NYHA I NYHA II NYHA IV NYHA III CAPRICORN COPERNICUS (Carvedilol vs Placebo): -23 % (Carvedilol vs Placebo): -35% US Carvedilol (Carvedilol vs Placebo):-65 % CIBIS II (Bisoprolol vs Placebo): -34% MERIT-HF (Metoprolol vs Placebo): -34% COMET (Carvedilol vs Metoprolol: -17 %)
COMET: Fakten zur Metoprolol Dosierung • In COMET wurde nicht retardiertes Metoprolol-Tartrat eingesetzt, Zieldosis 100 mg • Retardiertes Metoprolol-Succinat war zu Beginn der COMET (1996!) nicht verfügbar, die MERIT-HF Daten wurden erst 1999 publiziert • Die Bioverfügbarkeit von retardiertem Metoprolol-Succinat ist um 30-35% niedriger (Poole-Wilson et al. Lancet 2003) • In MERIT-HF wurde retardiertes Metoprolol-Succinat eingesetzt, Zieldosis 200 mg, dies entspricht ca. 130 mg Metoprolol-Tartrat (Poole-Wilson et al. Lancet 2003) • In MERIT-HF war die Mortalitätsreduktion in der Hochdosis-Gruppe (ø192 mg) gleich wie in der Niedrigdosis-Gruppe (ø76 mg) (Wikstrand et al. JACC 2002)
MERIT-HF: Effekt der Dosis auf die Mortalitätsrate Metoprolol-Succ. 76 mg/Tag Metoprolol-Succ. 192 mg/Tag 25 25 38% Risikored. P = 0.010 38% Risikored. P = 0.002 20 20 15 15 Placebo n = 1845 Placebo n = 1845 % Mortalität 10 10 Metoprolol Succ. n = 604 Metoprolol Succ. n = 1202 5 5 0 0 0 3 6 9 12 15 0 3 6 9 12 15 Months Months Wikstrand J et al. J Am Coll Cardiol 2002
MERIT-HF: Metoprolol-Dosisgruppen und Reduktion der Mortalität nach Wikstrand J. et al., JACC 2002;40:491-498
MERIT-HF: Reduktion der Mortalität in Abhängigkeit von der Dosis Nach Wikstrand J. et al., JACC 2002;40:491-498
HI-Erhebung bei 96 Ärzten in Ö: Betablocker Dosierung bei chron. HI in der Praxis Austrian Survey OF Treating Herat Failure, 2003, Prof. F. Fruhwald, Prof. P. Rehak, Graz




![The Indian Polycap Study (TIPS). Lancet 2009 Mar 30 [Epub]](https://cdn3.slideserve.com/6227256/slide1-dt.jpg)