Download
1 / 46
510 likes | 833 Views
DHIVA Dietitians in HIV/AIDS Group of the British Dietetic Association. Lipids and Lipodystrophy. Lisa Cooke MA BSc RD Head of Paediatric Dietetics Bristol Royal Hospital for Children. Lipids and Lipodystrophy.

E N D
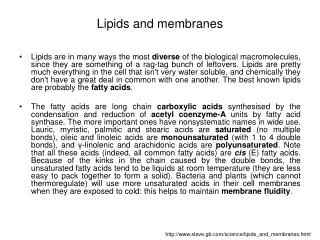
DHIVA Dietitians in HIV/AIDS Group of the British Dietetic Association Lipids and Lipodystrophy Lisa Cooke MA BSc RD Head of Paediatric Dietetics Bristol Royal Hospital for Children
Lipids and Lipodystrophy • Why are we interested in lipid levels and lipodystrophy when caring for children with HIV? • How are we monitoring in UK clinics? • What are the potential consequences for the children we manage in the UK? • Where do we go with lipid management for the children we care for in the future?
Why are we interested in lipid levels? • HIV Lipodystrophy Syndrome • HALS • HAART treatment Associated Lipodystrophy Syndrome
Lipodystrophy • Fat redistribution • Dyslipidaemia • Glucose Intolerance • Insulin Resistance
Lipoatrophy • Metabolic changes • Altered fat cell differentiation • Reduced lipogenesis • Fat loss in the periphery
Lipodystrophy • Adipocytokines(Adiponectin) • Reduced levels • Decreased insulin activity • Increased lipolysis • Increased NEFA
Lipohypertrophy Gynaecomastia Buffalo Hump
How are we monitoring in UK clinics? • Monitoring lipodystrophy • Nutritional Assessment • Height, weight & BMI • Waist, hip, thigh, calf circ’s • Biceps, Triceps, SS, SI SFT • Lipid & Insulin profile
WHO Child Growth Standards A growth chart for the 21st century
Royal College of Paediatrics and Child Health • UK-WHO Growth Charts • The RCPCH has launched new UK growth charts to plot weight, height and head circumference of children from birth to 4 years of age: • A4 growth chart 0-4 years • A5 growth charts for the Personal Child Health Record (PHCR) • A4 growth chart for hospitalised low birth weight infants 0-2 years • Charts and accompanying educational materials now available to download here.http://www.rcpch.ac.uk/#
Managing Dyslipidaemia • Available Guidelines • British Hyperlipidaemia Association (1996) • American Academy of Pediatrics (1998) • American Heart Association (2002) • American Academy of Pediatrics (2008) • Consensus Statement (1998) • National Cholesterol Education Programme
Lipodystrophy • Management of Dyslipidaemia • Total Cholesterol • LDL Cholesterol • HDL Cholesterol • TAG
Algorithm for Treatment of Dyslipidaemia Total Cholesterol (mmol/l) <4.4 Acceptable (75th percentile) 4.4-5.2 Borderline Non-Fasting Levels >5.2 High (95th percentile) Refer to Dietitian if reported on more than two occasions Obtain Fasting Measurement Consider Rx change Provide Advice on Diet and Physical Activity Total Cholesterol can be measured non fasting as recent dietary intake has little impact
LDL Cholesterol (mmol/l) <2.9 Acceptable (75th percentile) 2.9-3.4 Borderline Triglycerides (mmol/l) <2.2 Acceptable (75th percentile) Non-Fasting Levels Friedwald Equation Fasting TG <10.2 mmol/L LDL-C and HDL-C LDL-C >3.4 High (95th percentile) HDL-C < 0.9 TG >2.2 High (95th percentile) Refer to Dietitian if reported on more than two occasions Obtain Fasting Measurement Provide Advice on Diet and Physical Activity Achieve/maintain BWT N.B. TG >5.5 Very High Needs prompt treatment
DietaryIntervention • Cardioprotective diet • ( Age > 2 years) • Total fat ~30% daily energy • Saturated fat ~10% daily energy • PUFA & MUFA ~ 10% (N-3 and N-9)
Dietary Intervention • Cardioprotective diet • (> 2 years) • Less sugar • Fruit & Veg – 5 a day • Wholegrains • Soluble Fibre
Dietary Intervention • More strict after 3 months • Total fat ~ 20% • Saturated fat ~7% • Monitor regularly • Check growth and development
Consider Pharmacological Interventions In children > 10 yrs e.g. statins with LDL-C > 4.9 mmol/l or LDL-C > 4.1 with family history or > 2 additional CVD risk factors • Fasting Measurements TC Cholesterol 5.2 mmol/L LDL Cholesterol >3.4 mmol/L Triglycerides >2.2 High Plasma Insulin >20 mU/L? Cardioprotective Diet Increased Exercise Achieve/maintain healthy weight Review after 6-12 months
What are the potential consequences for the children we manage in the UK?
Obesity: A Global Epidemic • World Wide • 1.6 Billion Overweight • 400 Million Obese
Childhood Obesity • UK Prevalence(2006) • Age 2-15y • 31% (17%) boys • 29% (15%) girls Reception and year 6 measuring programme South West SHA 2007/8 Overweight- Reception -14%, Year 6 -14% Obese- Reception – 9%, Year 6 – 16%
Childhood Obesity • Trends • Foresight Report (2007) • 25% under 16’s obese by 2050 • Attributable cost to NHS £10 billion
Why does it happen? • Complex problem • Biological • Behavioural • Influenced by • Culture • Environment • Society
Why does it happen? • Risk factors in early life • Rapid growth in infancy • Weight gain in infancy • Weightgain in toddlers • One or both parents obese
Why does it happen? • Risk factors throughout life • Diet • Physical Activity • Sedentary Behaviours • TV viewing • Car use
Does it matter? • Obese children become obese adults • Tracks through childhood • Tracks into adulthood • Increased disease risk • Cardiovascular • Cancer • Respiratory • Psychological
What is being done? • Healthy Weight, Healthy Lives: A Cross Government Strategy for England (Jan 2008)
Eat Well, Move More, Live Longer DoH campaign From Jan 2009 http://www.nhs.uk/change4life/Pages/Default.aspx
Tailored clinical intervention • should be considered for children with a • BMI at or above the 91st centile, • depending on the needs of the • individual child and family. • Assessment of comorbidity • should be considered for children with a • BMI at or above the 98th centile. • Calculating BMI • Weight (kg) / Height m2 • Normal adult range = ~18-25 • Children Age and Sex specific • Must be plotted on centile charts
Where do we go with lipid management for the children we care for in the future?
Lipid Screening and Cardiovascular Health in Childhood Stephen R. Daniels, MD, PhD, Frank R. Greer, MD and the Committee on Nutrition PEDIATRICS 2008; 122; 198-208 doi:10.1542/peds.2008-1349
Extra recommendations • Impact of childhood obesity epidemic • Increased risk of cardiovascular disease in adulthood • Atherosclerosis established early in life • Identifed by vascular changes • Structure – Intimal Medial Thickness • Function – Flow Medicated Dilatation
Atherosclerosis linked to other CVD risk factors: • Age • Increased total serum cholesterol • Increased Low Density Lipoprotein Cholesterol • Reduced High Density Lipoprotein Cholesterol • Increased blood pressure • Obesity
Atherosclerotic process progressive • Clinical burden occurs in adulthood • Paediatric Healthcare Professionals • Greater awareness of CVD risk factors in childhood • Assess and monitor changes
Efficacy and Safety of Statin Therapy in Children With Familial Hypercholesterolemia A Randomized, Double-Blind, Placebo-Controlled Trial With Simvastatin Saskia de Jongh, et al for the Simvastatin in Children Study Group Circulation. 2002;106:2231. “Simvastatin significantly reduced LDL cholesterol, total cholesterol, triglycerides….and was well tolerated in children with heFH”
Drug Therapy of High-Risk Lipid Abnormalities in Children and Adolescents A Scientific Statement From the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee, Council of Cardiovascular Disease in the Young, With the Council on Cardiovascular Nursing Brian W. McCrindle et al Circulation. 2007;115:1948-1967 “In summary encouraging results have been obtained from clinical trials of statins in children and adolescents with familial or severe hypercholesterolaemia” Ultra long-term safety and compliance remain of concern
Why Mini DHIVA went to Mexico • Liaised with CHIVA- Piloting algorithms • Adults- Lipodystrophy and deranged lipids • What about children? • Obesity pandemic • Help!!
Where does Mini DHIVA go from here? • Annual Assessment audit • Collate data from this • Improve representation within CHIVA • Continue supporting KZN and other initiatives overseas • Production of ‘Nutrition and HIV’ textbook • Link up with Dietitians in the developing world • Use meetings to work together
Should we use drugs? • Numbers that would be eligible • How would it work • Expansion to other chronic diseases • HIV children in UK small population
Drug Interactions • Statins and PIs • Many contraindicated • Statins and NNRTIs • May need higher dose of statin • Limited data for children
Where do we go with lipid management for the children we care for in the future?