Download
1 / 37
390 likes | 910 Views
Fine Tuning Glaucoma Diagnosis and Management in Haiti. Daniel Laroche MD Director of Glaucoma, St Lukes -Roosevelt Hospital, NY President, Advanced Eyecare of New York Assistant Clinical Professor Ophthalmology New York Eye and Ear Infirmary New York Medical College

E N D
Fine Tuning Glaucoma Diagnosis and Management in Haiti Daniel Laroche MD Director of Glaucoma, St Lukes-Roosevelt Hospital, NY President, Advanced Eyecare of New York Assistant Clinical Professor Ophthalmology New York Eye and Ear Infirmary New York Medical College Chair NMA Ophthalmology Section/AAO Task for on Haiti Disclosure: Speaker Bureau for Alcon, Allergan Merck
Thanks to the SHO and CNPC for the invitation and congratulations on your ongoing efforts
Persistent Structural damage to buildings that need reconstruction
HUEH Faculty Dr. Jean Claude Cadet- Chief Dr. Ritza Eugene Dr. Jean Claude Cadet Jr. Dr. Valery Cadet Visiting Professors
Ophthalmology Residents Astrid St. Dic Rachel AglaeAmedee Rachel Gauthier Nathalie Francois Reginald Rejouis MyriamBeliard Marie Dieumane Chaperon MilonOsnel
3 ½ Days of seeing patients May 13-16, 2012 60 glaucoma patients were presented Under went tonometry, gonioscopy, optic disc examination, FDT VF Diagnosis were: Open angle glaucoma, Angle closure glaucoma, Juvenile Open angle glaucoma Traumatic Glaucoma, Congenital Glaucoma, Physiologic cupping without glaucoma, Congenital glaucoma, Neovascular glaucoma
Haitian Ophthalmology Residents Learning Gonioscopy www.gonioscopy.org
Residents Used Perkin tonometry to check IOP There was a shortage of slit lamps and goldmanapplanationtonometry available Only one 3 mirror gonio lens present Residents were trained to use the lens and also performed gonioscopy on each other Residents learned importance of optic disc drawings and were evaluated Each resident advised that they must invest in a four mirror lens to properly evaluate glaucoma
Resident Education Residents were given lectures on gonioscopy, optic disc evaluation, Target IOP in treating glaucoma, glaucoma surgical video were reviewed on trabeculectomy, trabeculotomy, Ahmed valve.
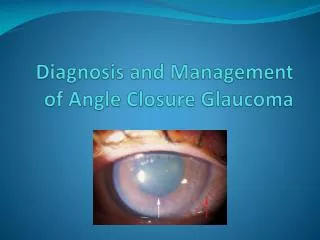
Allows viewing of angle structures when there is appositional Angle closure Angle will not open if Synechia is present Indentation Gonioscopy
Treatment for Angle Closure is iridotomy and sometimes with iridoplasty
2.4 1.9 1.4 Small Average Large Optic Disc Size • Size of cup varies with size of optic disc • Large optic discs have large cups in healthy eyes • Identify small and large optic discs • Small discs:avg vertical diameter < 1.5 mm • Large discs:avg vertical diameter > 2.2 mm
S N T I Look at the Neuroreintal rim: ISNT Rule Rim width: Distance between border of disc and position of blood vessel bending ISNT rule:Inferior > Superior > Nasal > Temporal
Notching Localized Rim Thinning/Notching
Patterns of Glaucomatous Progression 22% Disc cup enlargement Diffuse enlargement:round-shaped 56% Disc cup enlargementwith local notching Diffuse enlargement:vertically oval 9% Local notch Broader local notch 13% Pale neuroretinal rim;no change of configuration Pale rim; no changeof configuration Normal optic disc(left eye) First glaucomatousoptic disc change Type of progressionof disc abnormality Adapted from Tuulonen and Airaksinen. Am J Ophthalmol. 1991.
Localized Retinal Nerve fiber layer loss can be seen with red free light on ophthalmoscopy
Event Analysis, Look for VF progression was taught although only FDT available at the clinic Baseline Different from baseline?
AGIS 7Sustained IOP reduction below 18 mmHg is correlated with stability of visual field 5 Percent of Visits with IOP Less Than 18 mmHg 4 100% of visits 75 - 99% of visits 50 - 74% of visits 0 - 49% of visits MEAN IOP 20.2 mmHg 16.9 mmHg 14.7 mmHg 12.3 mmHg 3 2 Mean change in visual defect score 1 0 -1 0 1 2 3 4 5 8 6 7 Follow-up (years) AGIS Investigators, 2000, Am. J. Ophthalmol., 130, 429-440
Medical Management vs SurgeryBoth Stabilize Visual FieldsCollaborative Initial Glaucoma Treatment Study (CIGTS) 35%vs 48% IOP lowering Visual Field Score Time in Months 1- (reference IOP + VF score)/100 x Reference IOP =40% reduction Lichter et al, Ophthalmology, 2001 Nov: 108 (11) 1943-53
Ensuring Compliance With Antiglaucoma Treatment • Communication • More than 40% of pts being treated with glaucoma do not realize it can lead to blindness GRF survey • Education • Use the minimum number of medications required to safely achieve the target IOP • QD and BID dosing offers best compliance regimens • Non-compliance can be as high as 50% for one med, 61% for two meds, 70% for multiple meds Patel, Spaeth: Compliance in patients taking eyedrops for glauocma: Ophthalmic Surg 1995 26 ;3 ;233-236
Do not forget Laser and filtering surgery if medical therapy fails or ptscannot obtain medications.
Dr. Eugene to perform Ahmed valve with corneal patch with resident watching
Haitian Ophthalmology 2nd year Ophthalmology Residents performing trabeculectomy
Glaucoma Surgery 3 Ahmed valves performed 13 Trabeculectomies 3 pediatric examination under anesthesia 2 Trabeculotomy/Trabeculectomy
1st year residents watching 2nd year ophthalmology Residents performing glaucoma surgery
Congenital glaucoma with trabeculotomy under general Anesthesia at the University Hospital Main Operating Room Able to be performed
Still a great need for sutures, instruments, Glaucoma valves and patches, and medications Special thanks to New World Medical, Alabama Eye Bank, and Alcon. 1 tube inserter also donated
Glaucoma Challenges for developing World Compliance Cost (Medicaitons per month vsTrabeculectomy ) Lack of manpower Stigma associated with surgery Lack of glaucoma awareness Poor equipment maintenance Not enough visual rehabilitation programs
Potential Action items for Glaucoma Train a new generation of trainers in glaucoma subspecialty Encourage sandwich fellowships with physicians in the US and Canada Provide educational, training materials and resources from other countries and translate into French/Creole Systematically link professional development with institution capacity development Further develop and take advantage of online educational resources and link with HSO website www.web-sho.org
Towards the future in Haiti Important for eyecare providers and officials to ensure that glaucoma becomes a high priority along with cataracts as a treatable disease for blindness and to prevent blindness. We need continued development, refinement and validation of clinical and educational programs
Thank you Keep up the great efforts You are not alone Many are thinking of you and willing to work with you. I believe the private practice/public practice with sliding scale payments will succeed. Ongoing free eyecare by NGO’s undermines ophthalmology in Haiti Must support the residency program that is the future of ophthalmology in Haiti. Must support capacity in the ophthalmologists of HSO WITH LIMITED RESOURCES AND SUPPLIES COLLABORATION IS ESSENTIAL