Download
1 / 32
500 likes | 1.28k Views
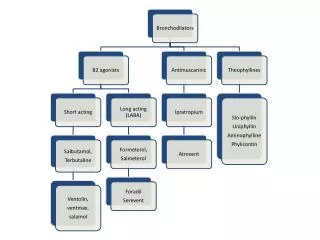
Pharmacology of Uterotonics. Uterotonics. Oxytocin Oxytocin Prostaglandin Ergot alkaloid Progesterone antagonist Tocolytics -adrenergist agonist Ca2+-channel blocker PG-synthase inhibitors Magnesium Sulfate Ethanol. Biosynthesis

E N D
Uterotonics Oxytocin • Oxytocin • Prostaglandin • Ergot alkaloid • Progesterone antagonist Tocolytics • -adrenergist agonist • Ca2+-channel blocker • PG-synthase inhibitors • Magnesium Sulfate • Ethanol
Biosynthesis • a cyclic non peptic, structurally similar to vasopressin • synthesized as a larger precursor molecul • rapidly broken down to the active hormone • packaged into secretory granules as and oxytocin-neurophysin complexs • secreted from nerve ending primarily in the posterior pituitary gland (neurohypophyses) Oxytocin
Physiologycal Roles Uterus • Stimulates contraction : frequency and force highly dependent on estrogen immature uterus : resistance • Responsiveness : paralel to spontaneous activity • Exogenous oxytocin : enhance rythmic contraction high dose for early pregnancy Breast • milk ejection
MOA • Oxytocin 1,4,5 triphosphate • mobilization Ca2+ intracellular • activation voltage-sensitive Ca2+ channels • Local prostaglandin production
Induction of labor (selected) • risk of continued pregnancy • isoimmunization • intrauterine growth retardation • placental insufficiency Clinical Use
Augmentation of labor • should not be used : progressing normally • hypotonic contraction in disfunctional labor • complication : trauma of the mother / fetoes • uterine rupture compromized fetal oxygenation • very prolong latent phase of cervical dilation • arrest / descent of dilation • epidural anesthesia
Third stage of labor and puerperium • after delivery or following therapeutic abortion • Oxytocin challenge test • pregnancy hold increased risk for maternal or fectal complication • Oxytocin receptor antagonists • competitively inhibit the interaction of oxytocin with its membran receptor • potential use in the treatment of preterm labor
HPETEs Prostaglandin
Inhibitors of Eicosanoid Biosynthesis • Calcium reducer • Glucocorticoids • NSAIDs • Analogs of the natural fatty acid precursores
Pharmacological Properties • Cardiovascular system prostaglandin tromboxan A2 leukotriens • Blood • Smooth muscle bronchial and tracheal uterus
continued PGFs TXA PGEs : relaxes Non pregnant : contractile > before menstruation relaxation > midcycle Pregnant : PGFs low concentration PGE2 high concentration PGE2 PGI2 iv PGE2 PGF2 contracted contracted relaxed Tone, frequency & intensity of rhytmic contraction >
continued • Gastric and intestinal secretion • Kidney and Urine Formation • Central Nervous System • Endocrine • Metabolic effects
Therapeutic uses • Therapeutic abortion abortifacients when given early in pregnancy dinoprostone (PGE2) misoprostol (PGE1) + mifepristone or methotrexate • Gastric Cytoprotection • Impotence • Maintenance of Patent Ductus Arteriosus
The Ergot Alkaloids Pharmacokinetic Absorption : variably from GI tract Oral dose of ergotamine 10x > im dose speed of absorption and peak blood level can be improved with caffeine Also absorbed from buccal cavity, rectum and after aerosol inhaler Metabolism : extensive
Pharmacodynamics A MOA : agonist partial agonist antagonist agonist at dopamine CNS receptor uterus : agonist / partial agonist at 5-HT2R B Organ system effects CNS Vascular smooth muscle Uterine smooth muscle Other smooth muscle at -adrenoceptor & serotonin receptor
Clinical Uses : A. Migraine B. Hyperprolactinemia C. Postpartum hemorrhage D. Diagnosis of Variant Angina E. Senile Cerebral Insufficiency
Toxicity : - gastrointestinal - medullary vomiting centre - prolong vasospasm * large doses of nitroprusside - fibroblastic changes * periodic drug holidays (methysergide) • Contraindication : - obstructive vascular diseases - collagen disease - (pregnancy)
Antiprogestins • Mifepristone (RU486) derivate of the 19-norprogestin norethindrone competitive antagonist of glucocorticoid and progesterone • Pharmacological actions : - antagonist progesterone - mifepristone - antagonist invivo - agonist invitro - onapristone - antagonist invivo & invitro
MOA : Mifepristone Early stage of pregnancy Decidual breakdown Detachment of the blastocyst h CG < Progesterone < PG > Contraction
Pharmacokinetics : - orally active - good bioavailability - peak plasma : several hours - H.L. : 20-40 hours - Binding 1 – acid glycoprotein - Liver metabolism & enterohepatic circulation - Excretion : > faeces
Therapeutic Uses : - Mifepristone termination early pregnancy + misoprostol - Mifepristone (48 hours) medical abortion T 1 + prostaglandin - Postcoital contraceptive
TOCOLYTICS treatment of Preterm Labor * bedrest * hydration * sedation (+ tocolytics)
- Adrenergic Agonists • Ritodrine • Terbutaline Tachycardia Hypotension Pulmonary edema Hypo kalemia Palpitation, tremor, Hyperglycemia angina
Therapeutic Uses • iv. to arrest premature labor • can prolong pregnancy
ETHANOL • Inhibit preterm labor • Overt inebriation • iv : impaired gag reflex • Carbohydrate metabolism more serious in diabetic • Crosses placenta
Prostaglandin Synthase Inhibitor • Inhibit labor • Oral / rectal endomethacin effective in the treatment of preterm labor • Serious potential ADR in the fetoes
Calcium Channel Blockers • Verapamil and nifedipine • Inhibition of premature labor • Nifedipine : - decreasing uterine contraction - severe dysmenorrhea - PG – induced abortion
Magnesium Sulfate • Inhibiting premature labor antagonizes Ca 2+ • Agent of choice in diabetic patients • Crosses placenta // maternal level • Respiratory depression in the mother : 10 ml of 10% calcium gluconate
Suggested for the Treatment of Preterm Labor • Diazoxide • Aminophylline • Progesterone