Download
1 / 23
230 likes | 373 Views
Reported Pertussis Among Adults Aged 65 Years and Older, Wisconsin, July 2011- December 2012 . Roman Aydiko Ayele, MPH Assistant Researcher Supporting the Wisconsin Department of Health Services University of Wisconsin - Madison School of Medicine and Public Health June 10, 2013.

E N D
Reported Pertussis Among Adults Aged 65 Years and Older, Wisconsin, July 2011- December 2012 Roman Aydiko Ayele, MPH Assistant Researcher Supporting the Wisconsin Department of Health Services University of Wisconsin - Madison School of Medicine and Public Health June 10, 2013
Disclosures Roman Aydiko Ayele, Ruth Koepke, and Ashley Richardson-Haleem are funded through the University of Wisconsin School of Medicine and Public Health by a grant from Sanofi Pasteur to collect pertussis case information for a phase IV DTaP relative effectiveness study that is unrelated to this study. James H. Conway is partially funded by the same grant from Sanofi Pasteur.
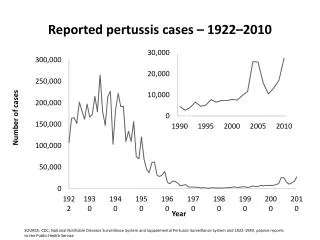
Background • Pertussis outbreaks have typically occurred at intervals of 3–4 years, with an increasing shift of disease burden among adults. 1 • Pertussis impacts activities of daily living (ADL)2and quality adjusted life years (QUALYs)among adults aged ≥65. 3 • Half of reported pertussis cases occur among adults and adolescents who serve as the major reservoir for spread to infants and younger children.4 • Pertussis is underdiagnosed and underreported, therefore the actual burden of disease among adults aged ≥65 is unknown. 5,6,7,8
Background continued • Challenges to diagnosing and reporting pertussis among all adults include: 9,10 • Under recognition of pertussis as a cause of cough illness. • Atypical presentation of signs and symptoms among adults. • Alow index of suspicion among some providers.
Background continued • ACIP recommends all adults aged ≥65 receive Tdap (February 2012). 11 • To reduce morbidity and mortality among this age group. • To reduce the transmission of pertussis to infants and in health-care settings. • Among adults aged19-64 years Tdap coverage rate was 12% during 2011.12 • Tdap has a safety profile similar to Td among adults and to Tdap among adolescent population (empirical safety data).13
Background continued • Paying for Tdap. • Tdap vaccine is not covered by Medicare Part A (Hospital Insurance) or Medicare part B (Supplementary Medical Insurance).14 • Medicare prescription drug plans (Part D) cover all commercially available vaccines (like the Tdap vaccine) needed to prevent illness.14 • 20% of Medicare Part D eligible individuals in WI have unknown creditable drug coverage.15
Agenda • Pertussis case investigation • 2011-2012 Pertussis Outbreak Summary, Wisconsin • Overview of pertussis among persons aged ≥65 years • Treatment • Vaccination • Clinical features/comparisons • Limitations • Conclusion • Recommendations
Pertussis case investigations • Local health departments investigate reported cases and report to DPH all cases (confirmed, probable, suspect, not a case) using the Wisconsin Electronic Disease Surveillance System (WEDSS): • Suspected cases of pertussis are reported directly by health care providers. • Positive PCR and/or culture test results reported electronically by labs. • Negative tests reported by labs on patients with pertussis symptoms. • All cases are categorized using the CSTE/CDC definitions for confirmed and probable.
Reported Pertussis, Wisconsin, July 1, 2011, to December 31, 2012 • 7454 reported cases with cough onset meeting CSTE/CDC case definitions. • confirmed cases: 5,322 (71.4%) • probable cases: 2,132 (28.6%) • Statewide Incidence: 130.7 cases per 100,000 population during the outbreak interval.
Number of reported confirmed and probable cases of pertussis by month and year of cough onset, Wisconsin, January 1, 2004, through December 31, 2012
Reported Pertussis occurring among persons aged ≥65 years with reported Pertussis, Wisconsin, July 2011-December 2012 • 149 confirmed and probable cases • 134 (95%) with laboratory test results • 87 (58%) confirmed cases • 79 (91%) of the cases were lab confirmed • 1 culture positive • 78 PCR positive • 8 (5%) epi linked confirmed cases • 4 linked to infectious children aged 8-13 years • 4 linked to infectious spouses • 62 (42%) probable cases
Demographic features of patients aged ≥65 years with reported Pertussis, Wisconsin, July 2011-December 2012 • Reported cases: 149 • Race: 79% White, <1 % multiple race, 20% unknown • Ethnicity: 74.5 % Not Hispanic or Latino, <1% Hispanic or Latino, 25% unknown • Age: Median 72 years (range:65 to 91 years) • Sex: 63% female, 36 % male, <1% unknown
Treatment and Vaccination • 133 (89%) patients reported receiving appropriate antibiotic treatment for pertussis. • Most received treatment the same day they were tested • 25 (17%) patients reported receiving Tdap. • Median years since vaccination: 1.7 years
Pertussis clinical features, Wisconsin, July 2011-December 2012
Pertussis clinical features, Wisconsin, July 2011-December 2012
Other features • When compared to pertussis patients aged <65 years, patients aged ≥65 years were: • Initially tested later after cough onset date (14 days vs. 11 days, P<0.01) • More likely to be females (63% vs. 53%, p <0.01)
Limitations Race and ethnicity information is incomplete, therefore unable to fully assess impact on different racial and ethnic groups. Insufficient data regarding types of residence (independent living, assisted housing, nursing home) for most of these patients. Re-hospitalization rates and most other complications that are reported as common in other studies of older adults with pertussis are unknown in our cohort.
Limitations • Sources of B. pertussisfor these patients is generally, unknown or not recorded. Frequency missing = 119
Conclusion Hospitalizations and pneumonia associated with pertussis are more common among adults aged ≥65 years. Apnea and other symptoms such as sleep disturbance hinder quality of life and could further complicate existing conditions such as asthma. Vaccination among this age group is recommended to prevent pertussis and possible B. pertussis transmission to other vulnerable family members.
Recommendations • Providers should: • Increase their index of suspicion for pertussis among patients aged ≥65 years with cough illness. • Encourage Tdap vaccination among individuals in this age group. (Don’t miss an opportunity!) • Educate patients in this age group about how pertussis can affect and exacerbate existing conditions such as asthma and sleep apnea. • Provide information regarding payment methods and resources for Tdap.
Acknowledgements • Wisconsin Division of Public Health, Bureau of Communicable Diseases and Emergency Response • Jeffrey P. Davis, MD • Daniel Hopfensperger, Immunization Program Manager • Stephanie Schauer, PhD • Ruth Koepke, MPH • Ashley Richardson-Haleem, MPH • University of WI School of Medicine and Public Health • James H. Conway, MD • Wisconsin Local Health Departments and Regional Representatives
References Quinn HE, McIntyre PB. Pertussis epidemiology in Australia over the decade 1995–2005 – trends by region and age group. Commun Dis Intell 2007;31(2):205–15. Schaffner W, Rehm SJ, and File TM Jr: Keeping our adult patients healthy and active: the role of vaccines across the lifespan. Phys Sports med 2010, 38(4):35–47. Eilers, Renske, et al. "Assessment of vaccine candidates for persons aged 50 and older: a review." BMC geriatrics 13.1 (2013): 32. Olyarchuk, Lizanne D., et al. "Examining the benefit of vaccinating adults against pertussis." Journal of the American Academy of Nurse Practitioners 24.10 (2012): 587-594. Cherry JD, Grimprel E, Guiso N, Heininger U, Mertsola J. Defining pertussis epidemiology: clinical, microbiologic and serologic perspectives. Pediatr Infect Dis J 2005;24(5 Suppl):S25–34. Cherry JD: The epidemiology of pertussis and pertussis immunization inthe United Kingdom and the United States: a comparative study. Curr Probl Pediatr 1984, 14:1–78. Jenkinson D: Duration of effectiveness of pertussis vaccine: evidence from a 10 year community study. BMJ 1988, 296:612–614. De Serres G, Shadmani R, Duval B, et al: Morbidity of pertussis in adolescents and adults. J Infect Dis 2000, 182:174–179. Hoffait M, Hanlon D, Benninghoff B, Calcoen S. Pertussis knowledge, attitude and practices among European health care professionals in charge of adult vaccination. Hum Vaccin 2011;7:197–201. Cornia PB, Hersh AL, Lipsky BA, Newman TB, Gonzales R. Does this coughing adolescent or adult patient have pertussis? JAMA 2010; 304:890–6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine in adults aged 65 years and older - Advisory Committee on Immunization Practices (ACIP), 2012., 2012. MMWR 2012; 61(25):468-70 http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6204a2.htm?s_cid=mm6204a2_w#tab1. Accessed 05/07/2013. Tseng, Hung Fu, et al. "Safety of a Tetanus-Diphtheria-Acellular Pertussis Vaccine When Used Off-Label in an Elderly Population." Clinical Infectious Diseases 56.3 (2013): 315-321. http://www.medicare.gov/coverage/tdap-vaccine-tetanus-diphtheria-and-pertussis-vaccine.html. Accessed 05/06/2013. http://kff.org/medicare/state-indicator/medicare-rx-drug-coverage/ Acessed 05/22/2013 Liu, Bette C., et al. "Pertussis in older adults: prospective study of risk factors and morbidity." Clinical infectious diseases 55.11 (2012): 1450-1456.