Download
1 / 23
240 likes | 588 Views
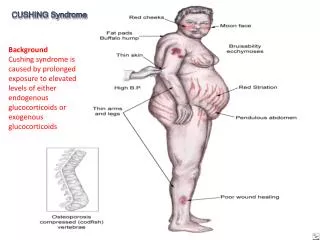
Paraneoplastic Cushing Syndrome. Wael Batobara. History. 52 y Male Smoker 30 pack Seen in Thoracic Sx Clinic with 1/12 H/O Chest Pain bilateral non pleuritic lower costal 4/10 not related to exertion No Fever ,Wt loss , Cough , Hemoptysis No Leg pain , swelling

E N D
ParaneoplasticCushing Syndrome Wael Batobara
History • 52 y Male Smoker 30 pack • Seen in Thoracic Sx Clinic with 1/12 H/O Chest Pain bilateral non pleuritic lower costal 4/10 not related to exertion No Fever ,Wt loss , Cough , Hemoptysis No Leg pain , swelling • Trail Of Abx & NSAID no effect
History • No SOB , Orthopnea , PND • Associated flank pain , No dysuria ,hematuria • PMH : -ve IHD risk factor • Works as Plumber , +ve exposure to asbestos • No Rx , travel
Examination • BP 150/80 HR 80 RR 18 Sat 93% Afebrile • Overweight • N JVP & cardiac exam • Chest N except bilateral tenderness lower ribs • ABD N ?LL edema
Investigations • CBC WBC 16 Neut.13 Hb .Coagulation N • Lytes , BUN & Creat. N • LFT Alk Phos 170 ALT 180 LDH 650 • Cardiac Enzymes & EKG N • CXR & Chest CT
Investigations • Brochoscopy edema Lt main Endobronchial lesion Sup.LLL • Mediastinoscopy Multiple LN • BAL & LN Bx Metastatic Small Cell CA • Bone Scan Diffuse skeletal Mets
The Story is not done Yet !!! Chest Medicine Has Not Been Involved Yet
This Should Have Been Picked Up Earlier R3 Medical Resident
New Complaint • Referred for work up of 1/12 H/O Bilateral Leg swelling Edema extending to Abdominal wall No New respiratory , cardiac symptoms No facial swelling NO decrease urine output , Leg Pain • Trial of Diuretics no improvement
Sequence Of Events • Patient was admitted to H6 • BP 150/85 • Not In CHF , No Signs of SVC obstruction • Pitting edema upto Ant Abd wall • No Leg Size Difference
Investigation • CBC & Coagulation N • Na 150 Co2 40 Cl ,BUN , Creat N • K 2.2 in spite of >300 meq daily supplement • FBS 8.1 Mg N • ABG PH 7.51 PAO2 65 PCO2 48 HCO3 41 • Metabolic abnormalities persists after stopping the diuretics
Investigation • CT Abd & Pelvis Multiple Mets Liver , spleen , kidneys Adrenal Looks Chubby No IVC obstruction • 2DE N LV & RV function • 24 Urine Collection High K
Investigation • Persistent Hypokalemia 2.3 EKG only U wave • Nephrology Consult {Please help it is your game} • Next day while rounding we caught Nephrology Staff Interesting Case!!!
24Hour Urine Cortisol 5250!!! Normal < 250
Hospital Course • Overnight Dexamethasone suppression test -ve Serum Cortisol 17501400 • ACTH pending • Oncology Consult Medical Resident Input Cis platinum & Etoposide • Endocrinology Ketoconazole
Investigation • Patient tolerated Chemo • Minimal K supplements with decrease CO2 • DM & HTN being treated • Follow up in Cancer Care
ParaneoplasticCushing Syndrome Incidence Is the presentation different from Cushing Dis. Would prognosis differ in SCLC with Cushing Is Chemothherapyis enough ? Other Paraneoplastic syndromes
Incidence • 20-30% of Cushing Synd. is 2ry to ectopic ACTH Lung Ca is the cause in 50% cases • Normal lung tissue secretes minimal amount of POMC proopiomelanocortin which is cleaved into different hormones including ACT { immunoreactive & not necessarily biologically active} • Up to 50% of Lung Ca will have High ACTH though 2-10% will have clinically significant disease
Incidence • 3 Retrospective studies SCLC had Cushing Synd • 14/840 1.6% Vs 5/157 3.2% Vs 10/126 2.6% • Dx clinical +High serum/urine cortisol • Majority Had extensive disease 60-90% • Cushing synd. Was diagnosed either with Ca Dx or shortly after Cancer Sept 81 & Mar 94 Arch Int Med Mar 93
Clinical Presentation • Less prominent than Cushing Disease shorter time of exposure to cortisol & the aggressive nature of tumor • Most common LL edema ,Muscle weakness & moon faces 40-60% • Most common lab finding Hypokalemia ,Met.Alk & Hyperglycemia 100%
Treatment • Majority required additional Rx to control hypercortosilemia • Worse consequence of febrile neutropenia in Patients whom hypercortisolemia was not controlled • Usual doses used to treat Cushing disease is not sufficient in Paraneoplastic Cushing • Rx used : Ketoconazole , Metyrapone ,Aminoglutethimide & Bilateral Adrenalectomy
Prognosis • SCLC with Cushing Synd, have a shorter survival rates than SCLC without the Synd. 4-6 months Vs 8-11 months • 3 reasons Larger tumor burden Relative lack of responsiveness to Chemo Tendency to develop serious infections • Infections common in patients with higher cortisol levels with different sites & pathogens