Download

1 / 15
150 likes | 252 Views
Effects of patient tracing on estimates of lost to follow-up, mortality and retention in antiretroviral therapy programs in low-middle income countries: a systematic review. James H. McMahon 1,2 , Julian H. Elliott 1,3,4 , Steven Y. Hong 2 , Michael R. Jordan 2

E N D
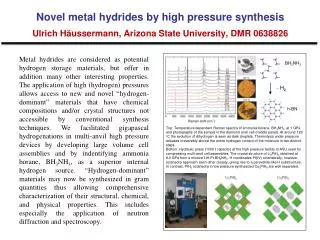
Effects of patient tracing on estimates of lost to follow-up, mortality and retention in antiretroviral therapy programs in low-middle income countries: a systematic review James H. McMahon1,2, Julian H. Elliott1,3,4, Steven Y. Hong2, Michael R. Jordan2 1Infectious Diseases Unit, Alfred Hospital, Melbourne, Australia; 2Department of Public Health and Community Medicine, Tufts University School of Medicine, Boston, Massachusetts, USA; 3Department of Medicine, Monash University, and 4Burnet Institute, Melbourne, Australia
Background • Frequently reported outcomes for populations receiving ART include the number of patients: • Alive and on ART • Died • Transferring care from one facility to another (‘transfer out’) • Stopping ART (physician directed or patient initiated) but remaining in care • Lost to follow-up (LTFU)
Background - Definitions • LTFU - generic term for patients initiating ART with unknown treatment outcomes • Unreported deaths • Unknown transfer of care without documentation • Disengagement from care • Retention on ART: patients alive and receiving ART 1 • Retained on ART = 1 – LTFU - died - stopped ART • Retention at the original site: individuals retained on ART and excludes transfers out 1 • Retained at the original site = 1 – LTFU – died – stopped ART – transfer out 1 Fox TMIH 2010, Rosen PLoS Med 2007
Background • Patient Tracing - Potential benefits: • Improved classification of unknown outcomes • Linking patients disengaged from care back into the health system • Methods of tracing: • Telephone tracing • Physical tracing • Prior reviews1 provide summary estimates of LTFU, mortality and retention but have not incorporated the potential for patient tracing to affect these outcomes Or combination of both 1 Fox TMIH 2010, Rosen PLoS Med 2007, Gupta PLoS One 2011, Lawn AIDS 2008
Objective • Compare summary estimates of LTFU, mortality and retention in low- and middle-income countries (LMICs) 12 months after ART initiation in cohorts of patients with and without physical tracing
Methods • Systematic review for studies in LMIC programmatic settings • MEDLINE (2003-2011) • HIV conferences (CROI and IAS 2009-2011) • MeSH and search terms for LTFU and retention • Included studies: reported proportion LTFU 12-months after ART initiation • Excluded studies: majority children, patients received mono- or dual-therapy, not performed in LMICs, clinical trials (non-programmatic setting)
Methods • Tracing activities determined from studies or contacting study authors • Classified as tracing study if physical tracing available for majority of patients • Summary estimates • Medians (IQR) if estimates non-normally distributed or; • Weighted means (± SD) if normally distributed • Weighting of proportions was by the inverse of its variance [1/(p x [1-p]/n); where p is proportion and n is sample size] • Compared by Student’s t-test if normally distributed, or Wilcoxon rank sum test if non-normal
Search strategy and study selection • Identified studies • 261 papers • Identified studies • 616 conference abstracts • Excluded after reviewing titles and abstracts • 149 papers • Excluded after reviewing titles • 334 conference abstracts • Full text review • 112 papers • Full text review • 282 conference abstracts • Excluded after reviewing full text • 80 papers • Excluded after reviewing • full text • 275 conference abstracts • Included in the review • 32 papers • Included in the review • 7 conference abstracts 32 papers and 7 conference abstracts included in the review
Comparison of summary estimates with and without physical tracing
Discussion • LTFU and mortality with physical tracing • Uncertain by how much the LTFU was a result of re-engagement into care versus re-classification of unknown outcomes • However, in addition to LTFU and mortality, we report in retention at the original site • Suggests tracing may re-engagement in care • Retention at the original site definition accounts for re-classification of lost patients as died or transferred out
Discussion • re-engagement would lead to beneficial effects of ART 1 • survival, fewer opportunistic infections, limiting treatment interruptions (minimizing emergence of HIV drug resistance), in community HIV viral load • Cost-effectiveness (CE) of tracing not known • Prior CE analyses on reducing LTFU have not considered tracing 2 1 Pallella NEJM 1998, Parienti CID 2004, Oyugi AIDS 2007, Das PLoS One 2010, Montaner JAIDS 2010, Andrews JID 2012. 2 Losina PLoS Med 2009
Discussion • Difference in summary estimates emphasizes the importance of knowing whether physical tracing occurs within an ART program or clinic when interpreting LTFU, mortality or retention data 1 1 2006 WHO IMAI guidelines, 2010 WHO HIVDR Early Warning Indicators, 2009 UNGASS indicators, 2009 PEPFAR indicators
Limitations • ART clinics with physical tracing may have resources resulting in improved outcomes • Review of randomized controlled trials (RCTs) with tracing interventions may provide more accurate assessments of the impact of tracing on LTFU, mortality and retention • RCTs not found Needed to quantify benefits and CE • Transfer out data available in a minority of studies • Estimates of retention at the original site could differ if complete transfer out data available • Emphasises the importance of understanding transfer out to accurately interpret estimates of retention
Conclusions • Physical tracing leads to: • unknown outcomes • Suggests improved re-engagement in care • Critical need for studies to assess tracing interventions for: • Ability to improve re-engagement of patients on ART • Optimal methods of tracing • Cost effectiveness • Programs providing ART in LMICs should consider physically tracing patients who have unknown outcomes as an intervention to improve individual outcomes and programmatic evaluation of populations receiving ART
Acknowledgements • Financial support • National Health and Medical Research Council • Postgraduate Scholarship - J.H.M • National Institutes of Health • 5K23AI074423-04 - M.R.J., 1K23AI097010-01A1 - S.Y.H. • In addition to study authors • Tufts Medical Center / Tufts University • Christine Wanke • Alfred Hospital / Monash University • Sharon Lewin • World Health Organization, HIV Department • Silvia Bertagnolio


![[ Ru (H)(H 2 )(PPh 2 CH 2 CH 2 PPh 2 ) 2 ] +](https://cdn2.slideserve.com/3881114/ru-h-h-2-pph-2-ch-2-ch-2-pph-2-2-dt.jpg)
![[SO 2 + H 2 O H 2 SO 3 ] SO 3 + H 2 O H 2 SO 4 CO 2 +H 2 O H 2 CO 3](https://cdn2.slideserve.com/4275035/slide1-dt.jpg)