Download
1 / 31
420 likes | 1.51k Views
Maternal Mental Health. Atif Rahman Daniela Fuhr. Maternal mental health.

E N D
Maternal Mental Health Atif Rahman Daniela Fuhr
Maternal mental health • Maternal mental health occurs in the antenatal (within pregnancy, i.e. before birth) and postnatal period (after giving birth, i.e. within first postnatal year) and most commonly presents as depression or anxiety disorders. However, it may also present with manic episodes and suicidal ideation.
Map displaying estimated prevalence of PND by country Parsons et al., 2011
Prevalence of non-psychotic common perinatal mental disorders • In low and middle income countries (LSICs): Prevalence of around 15% (95% confidence interval, CI: 15.4–15.9) antenatally and 19% (19.5–20.0) postnatally. • In high-income countries: Prevalence of around 10% antenatally and 13% postnatally. (Fisher, 2013)
Maternal mental health in India and Pakistan • The prevalence can be much higher in sub-communities or districts. • For instance, up to 20-25% of women in India and Pakistan can experience depression during pregnancy and after giving birth. Fisher, 2012
Risk and protective factors in LMIC Risk factors: • Socio-economic disadvantage: Living in poverty, unempoyment of husband, marital age (younger women), being unmarried/living in a polygamous marriage, belonging to a religious minority. • Family and social relationships: Intimate partner violence, no relationship with own family, higher number of children, conflict with in-laws (mother-in-law). Fisher, 2012
Risk and protective factors in LMIC 3) Reproductive and general health: Adverse reproductive events including unwanted or unintended pregnancy, past pregnancy losses, coincidental illness and operative birth. 4) History of mental health problems: Past psychiatric illness. 5) Infant characteristics: Sex of child, babies who cry alot, not latching on (difficulties with breast feeding), physical long-term illness of child. Fisher, 2012
Risk and protective factors in LMIC Protective factors: • More years of education. • Having a permanent or secure job. • Having an employed partner/husband. • Being a member of the ethnic majority. • Receiving traditional postpartum care from a trusted person (following traditional practices). Fisher, 2012
Impact of perinatal depression Impact on child: • Low birth weight • Growth restriction • Poor cognitive development • Higher risk of: • Stunted growth • Diarrhoeal episodes per year • Incomplete immunisation Impact on mother: • Increased risk of postpartum episode • Poor social functioning • Decreased productivity • Negative cognitions • Suicidal ideation Fisher et al., 2012; Bonari et al., 2004; Grote et al., 2010; Surkan et al., 2011; Rahman et al (2013); Patel et al, 2004 & Rahman, 2007.
What are the challenges to delivering a public-health level intervention for perinatal depression in LMIC?
18 Million women with perinatal depression180 psychiatrists1 psychiatrist to treat 1 Million women
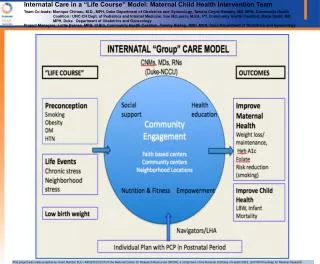
Interventions for maternal depression in LMIC Rahman et al (in press) Bulletin of WHO
The Thinking Healthy Programme (THP) A CBT intervention to reduce perinatal depression among mothers in Rawalpindi
The THP intervention in Pakistan: The Thinking Healthy Programme (THP) (Rahman et al, 2008) THP is a simplified CBT-based intervention: • Active listening, collaboration with family, guided discovery (questioning certain beliefs to generate new ideas) and homework. THP was developed for Lady Health Workers (LHWs): • LHWs are healthy mothers living in the same area as pregnant women with depression (peers). • They provide general maternal and child care/education in the community. • LHWs conducted 16 sessions, 4 in the prenatal period, 12 in the postnatal period till 8 months.
The Thinking Healthy Programme for Peer Delivery (THPP) Primary research objective: • To reduce the burden of depression in mothers by developing/evaluating the delivery of a brief psychological treatment (i.e. the THPP). • Adaptation of an intervention by Atif Rahman & colleagues (the Thinking Healthy Programme, THP). • THP was adapted so that it can be delivered by peers.
Lady Health Worker Programme • Largest community health worker programme in the world. • 100,000 LHWs covering all 135 districts of Pakistan. • 1 LHW for approximately 100-120 households. • Village-based, high school graduates with 6 months training and refresher courses. • Supervision – LHS.
Principles of ‘Thinking Healthy’ Programme • Child as the agenda. • Stress and burden rather than depression. • Integrated into community-based health worker’s (LHWs) routine work. • ‘Working together’ rather than therapy – to achieve child health. • Participatory. • Cognitive Behaviour Theory; Problem oriented; here and now –behaviour change communication.
Unhelpful thinking (cognitions) Unhelpful action (behaviour) The intervention: Cognitive Behavioural Therapy • “Cognitions” refers to our thoughts and “Behaviour” refers to our actions. • Cognitive Behaviour Therapy (CBT) is an evidence-based and structured form of talking therapy that aims to alter the cycle of unhelpful or unhealthy thinking (cognitions) and the resulting undesirable action (behaviour). Unhelpful emotions
Comparison of rates of DSM-IV Major Depression in intervention and control arms?
Outcomes of THP: Rates of depression at 6 and 12 months THP significantly lowered the rate of depression among mothers in the intervention group Rahman et al., 2008
Peers in low- to median-income countries (LMIC): other areas of health care • Peers have shown to be effective providers of health care in LMIC, facilitating mother and child programmes or care for non-communicable diseases. • Nepal and India: Significant reduction of neonatal mortality rate (Tripathy, 2010; Manandhar, 2004). • Bangladesh and Uganda: Improved initiation and duration of exclusive breastfeeding practices among mothers (Haider, 2000; Nankundu, 2006). • China: Peers led to significant improvements in diabetes patient’s self-efficacy as well as their systolic blood pressure (Liu, 2012) .
Implications for future research? • LMIC: Peer are an untapped resource in global mental health. • THPP trial is the first mental health trial on peers in LMIC. • Need to explore the use, applicability and effectiveness of other human resources to overcome the shortage of health professionals in mental health.