Download
1 / 44
470 likes | 628 Views
Thalassemias. Hemoglobin A. α. β. Fetal Hemoglobin (2 alpha, 2 gamma) Hemoglobin A2 (2 alpha, 2 delta) Small amounts in body. β. α. Disorders of Haemoglobin. 1. Thalassemia 2. Haemoglobinopathies. What is Thalassaemia ?.

E N D
Hemoglobin A α β • Fetal Hemoglobin (2 alpha, 2 gamma) • Hemoglobin A2 (2 alpha, 2 delta) • Small amounts in body β α
Disorders of Haemoglobin 1. Thalassemia 2. Haemoglobinopathies
What is Thalassaemia ? Thalassaemia is a group of inherited disorders of hemoglobin synthesis characterized by a reduced or absent one or more of the globin chains of adult hemoglobin . Genetic autosomal recessive blood disease. The name is derived from the Greek words Thalasso = Sea" and "Hemia = Blood" in reference to anemia of the sea.
Thalassemia • Mediterranean Anemia’- 1st published in 1925 • May be either homozygous defect or heterozygous defect.
Thalassemia • Results in overall decrease in amount of hemoglobin produced and may induce hemolysis. • May contribute protection against malaria.
Demographics: Thalassemia • Found most frequently in the Mediterranean, Africa, Western and Southeast Asia, India and Burma
GeneticTypesof Thalassaemia : There are two basic groups of thalassaemia. • Alpha ( )Thalassaemia • Beta ( )Thalassaemia
Clinical Types of Beta Thalassaemia : There are 3 types of Beta thalassaemia : • Thalassaemia Minor • Thalassaemia Intermediate • Thalassaemia Major
Genetics of Thalassemia • Adult hemoglobin composed two alpha and two beta chains. • Alpha thalassemia usually caused by gene deletion; Beta thalassemia usually caused by mutation. • Results in microcytic, hypochromic anemias of varying severity.
Gene Structure ( Alpha 1 and Alpha 2 produce identical chains)
Alpha Thalassemia • Alpha Thalassemia: deficient/absent alpha subunits • Excess beta subunits • Excess gamma subunits newborns • Tetramers formed: • Hemoglobin H adults • Hemoglobin Bart’s newborns • Five types: • Silent Carrier • Trait (Minor) • Hemoglobin H Disease • Major (Hemoglobin Bart’s) • Hemoglobin Constant Spring β/γ β/γ β/γ β/γ
Genetic basis of Alpha Thalassemia • Encoding genes on chromosome 16 (short arm) • Each cell has 4 copies of the alpha globin gene • Each gene responsible for ¼ production of alpha globin • 4 possible mutation states: • Loss of ONE gene silent carrier • Loss of TWO genes thalassemia minor (trait) • Loss of THREE genes Hemoglobin H • Accumulation of beta chains • Association of beta chains in groups of 4 Hemoglobin H • Loss of FOUR genes Hemoglobin Barts • NO alpha chains produced ∴ only gammachains present • Association of 4 gamma chains Hemoglobin Barts
Classification & TerminologyAlphaThalassemia • Normal / • Silent carrier - / • Minor -/- --/ • Hb H disease --/- • Barts hydrops fetalis --/--
Clinical Outcomes of Alpha Thalassemia • Silent carriers • asymptomatic • “normal” • Alpha Thalassemia minor (trait) • no anemia • microcytosis -unusually small red blood cells due to fewer Hb in RBC • “normal” • Alpha Thalassemia intermedia (“Hemoglobin H”) • microcytosis & hemolysis (breakdown of RBC)- results in severe anemia • bone deformities • splenomegaly (enlargement of spleen) • “severe and life threatening”
Clinical Outcomes of Alpha Thalassemia • Alpha Thalassemia major • Hb Bart’s • fatal hydropsfetalis- fluid build-up in fetal compartments, leads to death • occurs in utero
Beta Thalassemia • Beta Thalassemia: deficient/absent beta subunits • Commonly found in Mediterranean, Middle East, Asia, and Africa • Three types: • Minor • Intermedia • Major (Cooley anemia) • May be asymptomatic at birth as HbF functions
Genetic basis of Beta Thalassemia • Encoding genes on chromosome 11 (short arm) • Each cell contains 2 copies of beta globin gene • beta globin protein level = alpha globin protein level • Suppression of gene more likely than deletion • 2 mutations: beta-+-thal / beta-0-thal • “Loss” of ONE gene thalassemia minor (trait) • “Loss” of BOTH gene complex picture • 2 beta-+-thal thalassemiaintermedia / thalassemia major • 2 beta-0-thal thalassemia major • beta-+-thal / beta-0-thal thalassemia major • Excess of alpha globin chains
Classification & TerminologyBeta Thalassemia • Normal / • Minor /0 /+ • Intermedia0/+ +/+ • Major 0/0 +/+ 0/+
Clinical Outcomes of Beta Thalassemia • Beta Thalassemia minor (trait) • asymptomatic • microcytosis • minor anemia • Beta Thalassemiaintermedia • symptoms similar to Cooley Anemia but less severe • Beta Thalassemia major (Cooley Anemia) • most severe form • moderate to severe anemia • intramedullaryhemolysis (RBC die before full development) • peripheral hemolysis & splenomegaly • skeletal abnormalities (overcompensation by bone marrow) • increased risk of thromboses • pulmonary hypertension & congestive heart failure
Pathophysiology Disturbance of ratio between Alpha & non alpha globin chain synthesis then absent or decrease production of one or more globin chains Formation of abnormal Hb structures Ineffective erythropoiesis Excessive RBCs Destruction Iron Overload Extra-medullary hematopoiesis
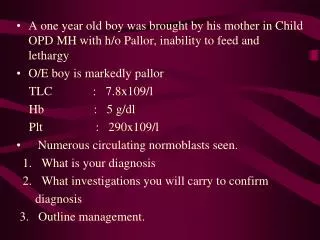
Signs & Symptoms • Thalassaemia Minor : Usually no signs or symptoms except for a mild anemia. • Thalassaemia Major : 1. Paleness, Jaundice or yellow coloured skin. 2. Growth retardation. 3. Bony abnormalities specially of the facial bones. 4. Enlarged spleen and liver.
Laboratory Diagnosis • Thalassemia minor: • Haemoglobin : Haemoglobin level is usually normal or mildly reduced. • Peripheral blood film : Hypochromia and Microcytosis (similar to Iron Deficiency Anemia). • MCV< 75 fl, RDW < 14%. • Reticulocyte Count increases • Decrease Osmotic Fragility • Haemoglobin electrophoresis • HPLC (High Performance liquid chromatography)
Other Special Procedures • Globin Chain Testing - determines ratio of globin chains being produced. • DNA Analysis - Determine specific defect at molecular DNA level.
Course and treatment of thalassaemia Untreated • thalassemia Major : Death in first or second decade of life • Intermedia: variable life span • Minor/Minima: Normal life span
Treatments for Alpha Thalassemia • Silent Carrier – no treatment required • Trait (Minor) – no treatment required • Hemoglobin H Disease – Folate • avoid iron supplements • Major (Hemoglobin Bart’s) –RBC transfusion while still in womb, else fetus is stillborn or dies shortly
Treatment for Beta Thalassemia • Trait – no treatment required • Intermedia • Major (Cooley anemia) • Regular folate supplementation • RBC transfusion (Splenectomy may decrease need for transfusions) • to maintain [Hgb] ~9-10g/dL • Blood transfusions iron accumulation iron overload • Iron chelators (diferroxamin)