Download
1 / 15
150 likes | 304 Views
Economic evaluation of outcomes: long term primary and surrogate endpoints. Dr. Giampiero Favato presented at the University Program in Health Economics Ragusa, 26-28 June 2008. Measuring health and disease. Many measures are used to assess health outcomes, ranging from:

E N D
Economic evaluation of outcomes: long term primary and surrogate endpoints Dr. Giampiero Favato presented at the University Program in Health Economics Ragusa, 26-28 June 2008
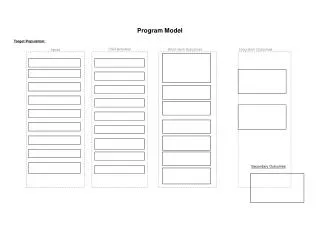
Measuring health and disease • Many measures are used to assess health outcomes, ranging from: • Those trying to capture the effect of an intervention on people’s general health (e.g. quality of life, Short Form36 (SF36) or days off work). • To: • Measures of a specific dimension relevant to a particular disease (e.g. peak flow rate). • People do not have the experience or knowledge of these conditions and the interventions to make accurate judgements as to the likely benefits. • Health care policy makers also need evidence on the likely benefits from health care spending (clinical evaluation) and whether these benefits justify the costs (economic evaluation). Primary endpoints Surrogate endpoints
Continuous vs. discrete outcomes measures • When the outcomes of a study are continuous (e.g. temperature, blood pressure, or cholesterol concentrations), the researchers are usually interested in the extent to which these values change after exposure to an intervention. • Instead of measuring health outcomes on a continuous scale, studies often focus on health events, such as cases of disease, death, or hospital discharge. What these outcomes have in common is that the event either occurs or it does not; they are discrete measures. Surrogate endpoints Primary endpoints
Components of economic evaluation Source: M. Drummond et al., Methods for the economic evaluation of health care programmes. Second edition. OUP 1997
Extrapolating health benefits from the short to the long term • For some health care interventions, such as antibiotic treatment for an acute infection, all the relevant benefits (and costs) occur over a relatively short period of time. • Many interventions are for diseases (that progress over time), such as Alzheimer’s disease or rheumatoid arthritis. In such cases the relevant time period for the economic evaluation could be a number of years. • If clinical studies always followed patients for a lifetime, there would be no need for extrapolation. However, long-term follow-up is costly and often infeasible, so some method of extrapolation is required in order to estimate health benefits over the relevant time period for economic evaluation.
Methods of extrapolation • Linking short and long-term outcomes via an epidemiological risk factor model. • Statistical extrapolations of survival curves. • State transition models, the most well-known of which is the Markov model (Briggs and Sculpher, 1998).
Example: cost-effective analysis of anti-HPV vaccination programme in Italy. • Study objective: to evaluate the cost-effectiveness of a multi-cohort vaccination strategy. • Perspective: the provider (Italian SSN) • Method: multi-cohort Markov model. Favato G. et al. Cost-effective analysis of anti-HPV vaccination programme in Italy: a multi-cohort Markov model. Henley discussion paper series. HCVI n° 13, February 2007
The model Favato G. et al. Cost-effective analysis of anti-HPV vaccination programme in Italy: a multi-cohort Markov model. Henley discussion paper series. HCVI n° 13, February 2007
year 1 year 2 year 3 year 4 year 5 year 6 11 17 age 12 13 14 15 16 17 18 25 age 19 20 21 22 23 24 Vaccination strategy • 11 year old cohort: reference • 4 options evaluated: • 2 cohorts (11-25 and 11-18 years) • 3 cohorts (11-18-25 years) • 4 cohorts (11-12-18-25 years)
11-12 years: still not exposed to HPV virus 18 years: age immediately before HPV infection peak 25 years: reduction of pre-cancerous lesions (integration with screening programme) Multi-cohort strategy
∆ = 5 ∆ = 19 ∆ = 31 Max theoretical reduction of HPV 16/18 induced carcinoma (%) Average reduction obtainable with screening programme Co-horts Results: 3-4 cohorts to obtain high efficiency in short-medium time
Cumulative reduction of all events (%) Events: erroneous Pap test, colposcopies, ASCUS, LSIL, HSIL, cervical cancer and genital condilomatosis anni 1 5 10 15 20 25 30 35 3-4 cohorts reduce the time to event reduction
Outcome Euro (Mill) savings incremental cost Break-even reached after 8 years Overall cost reduction > 50% years Favato G. et al. Cost-effective analysis of anti-HPV vaccination programme in Italy: a multi-cohort Markov model. Henley discussion paper series. HCVI n° 13, February 2007
Dealing with uncertainty: sensitivity to cervical carcinoma in different ethnic groups