Download
1 / 40
480 likes | 615 Views
Acute Leukemia Samed Al-Ameri, BSc MLT. Headline. Definition Etiology Pathophysiology Classification Clinical Manifestations Diagnostic Studies. Leukemia Definition. A group of malignant disorders affecting the blood and blood-forming tissues of Bone marrow Lymph system Spleen

E N D
Headline • Definition • Etiology • Pathophysiology • Classification • Clinical Manifestations • Diagnostic Studies
Leukemia Definition • A group of malignant disorders affecting the blood and blood-forming tissues of • Bone marrow • Lymph system • Spleen • Results in an accumulation of dysfunctional cells because of a loss of regulation in cell division
Leukemia Etiology • No single causative agent • Most from a combination of factors: • Genetic and environmental influences • Chemical agents • Chemotherapeutic agents • Viruses • Radiation • Immunologic deficiencies
Stage 1- Normal Stage 2- Symptoms Stage 3- Diagnosis Stage 5a- Anemia Stage 4- Worsening Stage 5b- Infection Development of Leukemia in the Bloodstream Legend White Cell Red Cell Platelet Blast Germ Sources from Leukemia, by D. Newton and D. Siegel
leukemia Classification Main classification Acute leukemia Chronic leukemia Lymphoid (CLL) Myeloid (CML) Lymphoid (ALL) Myeloid (AML)
FAB criteria Morphology Cytochemistry WHO criteria Morphology Immunophenotyping Genetic features Karyotyping Molecular testing Clinical features Acute LeukemiaClassifications FABvs. WHO
Acuteleukemia FAB Classification (1976) Acute leukemia Lymphoid (ALL) Myeloid (AML) L1 Homogenous small lymphoblasts; mostly in children L2 Large heterogeneous blasts; mostly in adults L3 -Burkett's large basophilic B-cell blasts with vacuoles M0 - Undifferentiated M1myeloblastic undifferentiated M2myeloblastic with differentiaion M3promyelocytic M4myelomonocytic M5monoblastic M6erythroleukaemia M7megakaryoblastic
WHO Classification of AML • AML with recurrent genetic abnormalities • AML with multilineage dysplasia • AML therapy related • AML not otherwise categorised • AML of ambiguous lineage
ALL germinal center B-lymphocytes Plasma cells Lymphoid progenitor T-lymphocytes Neutrophils AML Myeloid progenitor Eosinophils Hematopoietic stem cell Basophils Monocytes Platelets Red cells
Signs and Symptoms • Most of the signs and symptoms are due to: 1-Anemia. 2-Leukopenia. 3-Thrombocytopenia. • Bicytopenia, Pancytopenia. • All symptoms associated with leukemia can be attributed to other diseases, consequently, leukemiais always diagnosed by laboratory investigations.
Acute Lymphoblastic Leukaemia • Cancer of the blood affecting the white blood cell known as LYMPHOCYTES. • Commonest in the age 2-10 years • Peak at 3-4 years. • Incidence decreaseswith age, and a secondary rise after40 years. • In children - most common malignant disease • 85% of childhood leukemia
Acute Lymphoblastic Leukemia • Specific manifestation : *Bone pain, arthritis * Lymphadenopathy *Hepatosplenomegaly *Mediastinal mass *testicular swelling *Meningeal syndrome
Acute Myeloid Leukemia • Arise from the malignant transformation of a myeloid precursor • Rare in childhood (10%-15%) • The incidence increases with age • 80% in adults • Most frequent leukemia in neonate
Acute Myeloid Leukemia • Specific manifestation : - Gum hypertrophy • Hepatosplenomegaly • Skins deposit • Lymphadenopathy • Renal damage • DIVC mainly in (M3)
Diagnostic Studies Diagnosis • Morphology • Cytochemistry • Immunophenotyping • Cytogentics
Laboratory Findings CBC: • WBC:60% of pts have an elevated WBC. WBC count in acute leukemia can be high, normal, or low. ALL: • WBC usually elevated (20,000- 100,000 / cmm ). • 20% of pts have 50,000 / cmm • 90%have blast in the peripheral blood film. AML: • Median WBC count in AML is 15000/ cmm. • 20% of patients have > 100,000/cmm. • 25-40% of patients have <5000/cmm. • 95% of patients have blast cells on blood film. • Most are anemic, Anemia (normochromic, normocytic) • Most are thrombocytopenic, Thrombocyte <100,000/mm3
Laboratory Findings • Electrolytes: • Hypo/hyper kalemia • Hypomagnesaemia • hyperphosphatemia • Hypermetabolism: • LDH. • uric acid. • Abnormal Coagulation Test (DIC) • LFT, RFT
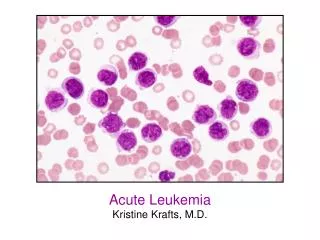
Platelet Platelet White Cell Red Cell Red Cell Blasts White Cell Normal human blood Blood with leukemia Pictures Of Blood Sources from beyond2000.com Sources from Arginine.umdnj.edu
Bone marrow biopsy and aspirate: • 20%or more of all nucleated cells are blast. • ALL (Lymphoblast) • Blast size :small • Cytoplasm: Scant • Chromatin: Dense • Nucleoli :Indistinct • Auer-rods: Never present • AML (Myeloblast) • Large • Moderate • Fine, Lacy • Prominent • Present in 50%
Bone marrow smear Normal Bone marrow ALL AML
The Cytochemistry ______________________ALL____________AML__________ • Myeloperoxidase - + • Suddan black - + • Non-specific esterase - + in M4, M5 • Periodic acid Schiff (PAS) + in c-ALL + in M6 • Acid phosphatase + in T-ALL + in M6
The Cytochemistry Periodic acid Schiff (PAS) positive ALL Peroxidase positive AML Acid phosphatase -focal positive (T-ALL)
AML CD13 CD33 CD34 Glycophorin M6 Platelet Antigen M7 ALL B lineage CD19 CD22 CD10 T lineage CD7 CD3 CD2 CD5 Immunophenotyping
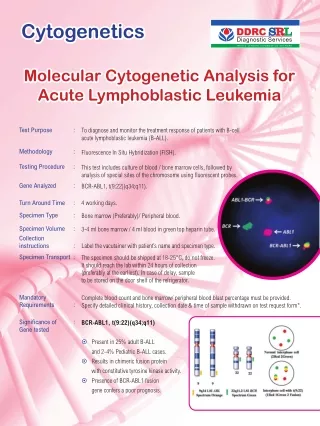
Cytogentics • Chromosomal abnormalities are found in the blasts in 70% of cases of AML and 90% of ALL • Important in the pathogenesis of the disease • Important for diagnosis • Prognostic implication
Cytogentics Common Chromosome Abnormalities Associated With Acute Leukemia • t(8;21) AML with maturation (M2) • t(15;17) AML-M3(APML) • Inv 16 AML-M4 • t(8;14) B-ALL • t(9;22) Chronic granulocytic leukemia • The Philadelphia chromosome : the product of a translocation between chromosomes 9 and 22 -confers a very poor prognosis in ALL.
Treatment • Supportive treatment • Chemotherapy • Blast Cell Transplantation