Download
1 / 12
120 likes | 245 Views
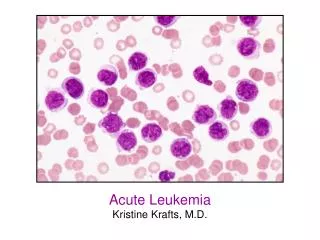
Acute Leukemia and the FLT3 Receptor. By: Betty Sa’ Mentor: Dr. Govind Bhagat Site: Columbia University Vanderbilt Clinic. BACKGROUND.

E N D
Acute Leukemia and the FLT3 Receptor By: Betty Sa’ Mentor: Dr. Govind Bhagat Site: Columbia University Vanderbilt Clinic
BACKGROUND • Leukemia is a cancer of the blood in which immature hematopoietic cells proliferate in an uncontrolled manner. Leukemia originates in the bone marrow and quickly spreads elsewhere. There are four major types of Leukemia, Acute Myeloid Leukemia (AML), Acute Lymphoblastic Leukemia (ALL), Chronic Myeloid Leukemia, and Chronic Lymphocytic Leukemia. But we are only focusing on AML and ALL. Acute means that the disease appears quickly and advances rapidly, so patients with ALL and AML usually require immediate treatment.
INTRODUCTION • Acute Lymphocytic Leukemia (ALL) is a rapidly progressing disease marked by the overabundance of immature lymphoid cells (lymphoblasts) in the blood or bone marrow; most commonly found in children. Healthy lymphocytes fight bacterial and viral infections. But in patients with ALL the lymphocytes do not develop into mature cells, and remain immature cells called lymphoblasts. In this type of Leukemia blood cells differentiation and gets stuck at the lymphoblast stage and continues proliferation. So the abnormal cells crowd the normal cells in the bone marrow and prevent the production of red blood cells, other white blood cells, and platelets. This causes most ALL patients to become anemic, susceptible to infection, and bruise or bleed easily. • Acute Myeloid Leukemia (AML)is a cancer in which there is uncontrollable growth of immature myeloid cells (myeloblasts, promyelocytes, monoblasts, erythroblasts, megakaryoblasts) in the bone marrow that leads to a deficiency of red blood cells, platelets, and white blood cells. In these types of Leukemia blood cell differention gets stuck at various stages of myeloid, monocytic, erythroid, or megakaryocytic differentiation and these cells continue to proliferate.
INTRO CONTINUES... • There are different sub-types of AML, depending upon exactly which type of cell has become leukemic the stage of maturation the cells are at and whether the cells are differentiated, these sub-types include: Acute Myeloid Leukemia without maturation, Acute Myeloid Leukemia with maturation, Acute Promyelocytic Leukemia (APL), Acute Myelomonocytic Leukemia, Acute Monocytic/Monoblastic Leukemia, Acute Erythroleukemia, and Acute Megakaryoblastic Leukemia. • In AML where the granulocytic (neutrophilic) series is affected, there is a block in the production of mature neutrophils. Neutrophilis fight infections caused by bacteria. The production of mature neutrophilis is usually tightly regulated. Mature neutrophilis develop from less mature white cells in a process called differentiation. In AML, acquired mutations in the blood-forming cells disrupt the normal process of differentiation, resulting in the accumulation of large members of immature cells called myeloblasts. If the erythroid lineage is affected, blasts cannot function like fully developed, healthy red blood cells. The large number of blasts also reduces the production of healthy red blood cells and platelets. So, patients are usually anemic.
ALL AML
FLT3 • FLT3 stands for FMS-like tyrosine kinase 3 gene, which encodes a membrane-bound receptor tyrosine kinase (RTK) that has a crucial role in normal haematopoiesis. • Normally, FLT3 expression is restricted to CD34+ hematopoietic stem/progenitor cells, brain, placenta, and gonads. Activation of FLT3 by FLT3-Ligand promotes the normal, in vitro growth of early progenitor cells. • In Acute Leukemia, mutations of the FLT3 gene have been found to be one of the most common acquired genetic lesions. FLT3 mutations can be detected in 30% of AML patients. There are two frequent types of somatic FLT3 genetic mutations: internal tandem duplications (ITDs) in the juxtamembrane (JM) domain and point mutations in the activation loop of the tyrosine kinase domain (TKD). • Studies have shown that ITD mutations are triggered by any elongation or shortening of the JM domain of FLT3 due to additions or deletions of amino acids that result in the constitutive activation of FLT3. The presence of FLT3/ITD mutations is associated with a poor clinical outcome in both pediatric and adult patients with AML.
FLT3 Continues... • Point mutations in the activation loop of the kinase domain (FLT3/TKD) involves the aspartic acid, D835 residue, which leads to an activated configuration and transformation of myeloid cells. D835 mutations are missense mutations that results in substitution of tyrosine, histidine, valine, glutamic acid or asparagine for aspartatic acid at amino acid 835 of FLT3. • This mutation has been reported in 7% of patients with AML. TKD mutations, unlike ITD mutations, have not been shown to have any prognostic significance in AML patients. • Both types of FLT3 mutation cause ligand-independent activation of the receptor and activation of downstream signaling pathways.
Statistics • In 2006 an estimated 3,930 adults (2,150 men and 1,780 women) in the US will be diagnosed with ALL and an estimated 1,490 (900 men, 590 women) deaths will occur. ALL is more common in adults older than 50. 20% to 30% of adults with ALL experience long-term disease remission or are cured of the disease. • ALL is more common in children than in adults; 74% of all new cases are diagnosed in children ages 0 to 19. • In 2006, an estimated 11,930 people (6,350 men and 5,580 women) in the US will be diagnosed with AML and an estimated 9,040 deaths will occur (5,090 men and 3,950 women). AML is most common in older adults around 60-65 years old. • The percentage of patients who survived at least five years after being diagnosed, for adults under the age 65 with AML is 33%.
PURPOSE • To get a better understanding of the molecular abnormalities underlying Acute Leukemia's. • I will study the different types of FLT 3 tyrosine kinase mutations in subsets of acute leukemias to determine their relative frequency and impact on the biologic course of disease . • I will also correlate the presence of FLT3 mutations with other cytogenetic abnormalities in different types of acute leukemias to better understand the multi-step pathways of leukemogenesis.
Case selection – Acute leukemias diagnosed at Columbia University Medical Center over the past 5 years for which cytogenetic information is available (at least 100 cases) DNA extraction from peripheral blood or bone marrow aspirate samples PCR using primers specific for certain portions of the FLT3 gene Capillary gel electrophoresis Analysis of spectrophoretograms for FLT3 TKD and FLT3-ITD mutations Material and Methods
REFERENCES • http://www.dsrct.demon.co.uk/cells.jpg • www.nature.com/reviews/cancer • www.vghtpe.gov • www.health.sa.gov.au/cancare • www.elsevier.com/locate/biocel • www.sciencedirect.com • health.on-topic.net/health/Acute+Lymphocytic+...
Acknownledgements • Dr.Govind Bhagat • Dr. Mahesh Mansukhani Columbia University • Dr. Sat MSKCC • Harlem Children Society