Download
1 / 1
20 likes | 128 Views
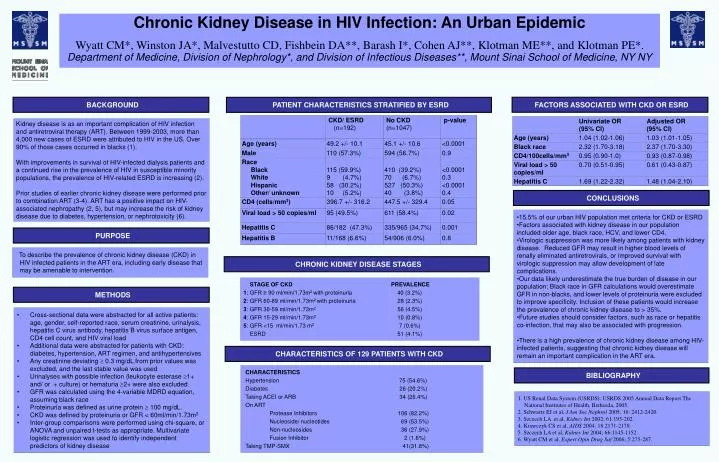
Chronic Kidney Disease in HIV Infection: An Urban Epidemic Wyatt CM*, Winston JA*, Malvestutto CD, Fishbein DA**, Barash I*, Cohen AJ**, Klotman ME**, and Klotman PE*. Department of Medicine, Division of Nephrology*, and Division of Infectious Diseases**, Mount Sinai School of Medicine, NY NY.

E N D
Chronic Kidney Disease in HIV Infection: An Urban Epidemic Wyatt CM*, Winston JA*, Malvestutto CD, Fishbein DA**, Barash I*, Cohen AJ**, Klotman ME**, and Klotman PE*. Department of Medicine, Division of Nephrology*, and Division of Infectious Diseases**, Mount Sinai School of Medicine, NY NY FACTORS ASSOCIATED WITH CKD OR ESRD BACKGROUND PATIENT CHARACTERISTICS STRATIFIED BY ESRD Kidney disease is as an important complication of HIV infection and antiretroviral therapy (ART). Between 1999-2003, more than 4,000 new cases of ESRD were attributed to HIV in the US. Over 90% of those cases occurred in blacks (1). With improvements in survival of HIV-infected dialysis patients and a continued rise in the prevalence of HIV in susceptible minority populations, the prevalence of HIV-related ESRD is increasing (2). Prior studies of earlier chronic kidney disease were performed prior to combination ART (3-4). ART has a positive impact on HIV-associated nephropathy (2, 5), but may increase the risk of kidney disease due to diabetes, hypertension, or nephrotoxicity (6). CONCLUSIONS • 15.5% of our urban HIV population met criteria for CKD or ESRD • Factors associated with kidney disease in our population included older age, black race, HCV, and lower CD4. • Virologic suppression was more likely among patients with kidney disease. Reduced GFR may result in higher blood levels of renally eliminated antiretrovirals, or improved survival with virologic suppression may allow development of late complications. • Our data likely underestimate the true burden of disease in our population: Black race in GFR calculations would overestimate GFR in non-blacks, and lower levels of proteinuria were excluded to improve specificity. Inclusion of these patients would increase the prevalence of chronic kidney disease to > 35%. • Future studies should consider factors, such as race or hepatitis co-infection, that may also be associated with progression. • There is a high prevalence of chronic kidney disease among HIV-infected patients, suggesting that chronic kidney disease will remain an important complication in the ART era. PURPOSE To describe the prevalence of chronic kidney disease (CKD) in HIV infected patients in the ART era, including early disease that may be amenable to intervention. CHRONIC KIDNEY DISEASE STAGES STAGE OF CKD PREVALENCE 1: GFR ≥ 90 ml/min/1.73m2 with proteinuria 40 (3.2%) 2: GFR 60-89 ml/min/1.73m2 with proteinuria 28 (2.3%) 3: GFR 30-59 ml/min/1.73m2 56 (4.5%) 4: GFR 15-29 ml/min/1.73m2 10 (0.8%) 5: GFR <15 ml/min/1.73 m2 7 (0.6%) ESRD 51 (4.1%) METHODS • Cross-sectional data were abstracted for all active patients: age, gender, self-reported race, serum creatinine, urinalysis, hepatitis C virus antibody, hepatitis B virus surface antigen, CD4 cell count, and HIV viral load • Additional data were abstracted for patients with CKD: diabetes, hypertension, ART regimen, and antihypertensives • Any creatinine deviating 0.3 mg/dL from prior values was excluded, and the last stable value was used • Urinalyses with possible infection (leukocyte esterase 1+ and/ or + culture) or hematuria 2+ were also excluded • GFR was calculated using the 4-variable MDRD equation, assuming black race • Proteinuria was defined as urine protein 100 mg/dL. • CKD was defined by proteinuria or GFR < 60ml/min/1.73m2 • Inter-group comparisons were performed using chi-square, or ANOVA and unpaired t-tests as appropriate. Multivariate logistic regression was used to identify independent predictors of kidney disease CHARACTERISTICS OF 129 PATIENTS WITH CKD CHARACTERISTICS Hypertension 75 (54.6%) Diabetes 26 (20.2%) Taking ACEI or ARB 34 (26.4%) On ART Protease Inhibitors 106 (82.2%) Nucleoside/ nucleotides 69 (53.5%) Non-nucleosides 36 (27.9%) Fusion Inhibitor 2 (1.6%) Taking TMP-SMX 41(31.8%) BIBLIOGRAPHY 1. US Renal Data System (USRDS): USRDS 2005 Annual Data Report.The National Institutes of Health, Bethesda, 2005. 2. Schwartz EJ et al, J Am Soc Nephrol 2005; 16: 2412-2420. 3. Szczech LA et al, Kidney Int 2002; 61:195-202. 4. Krawczyk CS et al, AIDS 2004; 18:2171-2178. 5. Szczech LA et al, Kidney Int 2004; 66:1145-1152. 6. Wyatt CM et al, Expert Opin Drug Saf 2006; 5:275-287.