Download
1 / 22
240 likes | 532 Views
Lymphedema, Venous Stasis and the Importance of Compression. Timothy A. Hursh , MD Medical Director, Wound Care Kindred Hospital San Antonio. Agenda for Today’s Discussion. Physiology Diagnosis Clinical Presentation Treatment Case Examples. Physiology.

E N D
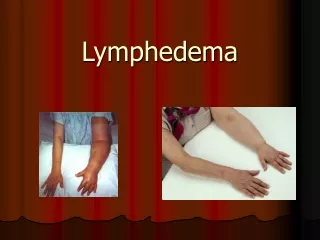
Lymphedema, Venous Stasis andthe Importance of Compression Timothy A. Hursh, MD Medical Director, Wound Care Kindred Hospital San Antonio
Agenda for Today’s Discussion • Physiology • Diagnosis • Clinical Presentation • Treatment • Case Examples
Physiology • Lymphedema (lymphatic obstruction) • Swelling due to blockage of the lymph channels • Causes include • Infection with parasites (filariasis) • Injury • Radiation • Surgery (mastectomy) • Radiation Therapy • Infection (cellulitis)
Physiology • Venous Stasis (aka Venous Insufficiency) • Veins unable to help blood return to the heart • Causes include: • One or more deep leg veins are compromised • “One-way-valves” either broken or missing • Risk factors include: increased age, history of leg DVT, female, increased height, pregnancy, obesity, prolonged sitting/standing
Diagnosis • Lymphedema • CT or MRI • Lymphangiogram • Lymphoscintigraphy (radioactive tracing) • Venous Stasis • Clinical diagnosis
Clinical Presentation • Lymphedema • Swelling of arm/leg (acute or chronic) • Staging • Stage 0 – lymph vessels damaged but are coping • Stage 1 – non-pitting edema, skin bounces back • Stage 2 – pitting tissue, hardening of skin begins & increased size • Stage 3 – lymphatic channels closed from fibrosis, limbs become swollen, hard
Clinical Presentation • Venous Stasis • Pts c/o dull aching, or cramping, limbs • Itching or tingling • Pain worse with standing, better with legs raised • Leg swelling • Chronic changes include redness, varicose veins, color changes around distal leg/ankles (bronzing), ulcers
Treatment • Lymphedema • Manual lymph drainage • Compression wraps • Light exercise (milking action of muscles) • Skin care to decrease risk of infection • Lymphedema pumps
Treatment • Venous Stasis • Compression wraps • No long periods of standing/sitting • Exercise • Wound care if wounds/ulcers
Treatment • Compression Wraps • Class I 20-30 mmHg • Class II 30-40 mmHg • Class III 40-50 mmHg • Class IV > 50 mmHg • Application should be done carefully from distal to proximal, midpoint overlapping, no wrinkles
Treatment Unnas Boot Profore • Common Types of Compression Wraps • ALWAYS APPLIED DISTAL TO PROXIMAL • Package instructions are not a “suggestion” • Spiral versus Figure 8 • Dry versus medicated • $$$ Can get costly very quickly • Are ACE wraps ok? • Ensure patients have after hours instructions
Case Example #1 • 68 yo male with 30 year Hx venous ulceration RLE • Obese, DM II, HTN • Meds: metformin, diuretics (taken only intermittently) • Tx included: Unna boot healed earlier; compression therapy at home but non-compliant so placed in compression stockings
Case Example #1 • Lived with ulcers for 4 years • Finally consented to treatment with combination of: • Exercise (dorsiflexion emphasized) • Alginate dressings covered with foam and light compression • After 6 weeks of COMPLIANCE………
Case Example #2 • 54 yo male with 5 yr Hx chronic lymphedema • PMH: Avascular necrosis of the hips, HTN, EtOH abuse, liver cirrhosis, chronic Hep C • Admitted for care of Stg 3 pressure ulcer of buttocks and newly developed ulcers of legs secondary to worsening lymphedema
Case Example #2 Jan 2012
Case Example #2 • Treatment consisted of wound care, debridements PRN, manual massage, compression wraps, exercise • Discharged after 4 weeks care with plans for clinic follow-up and HHC for daily treatment of his lymphedema • Condition at discharge………...
Case Example #2 Feb 2012
Thank You for Attending! • Contact Information: • Tim Hursh, MD • Kindred San Antonio • Medical Director for Wound Care • (210) 616-0616 • Timothy.Hursh@kindredhealthcare.com