Download
1 / 10
100 likes | 298 Views
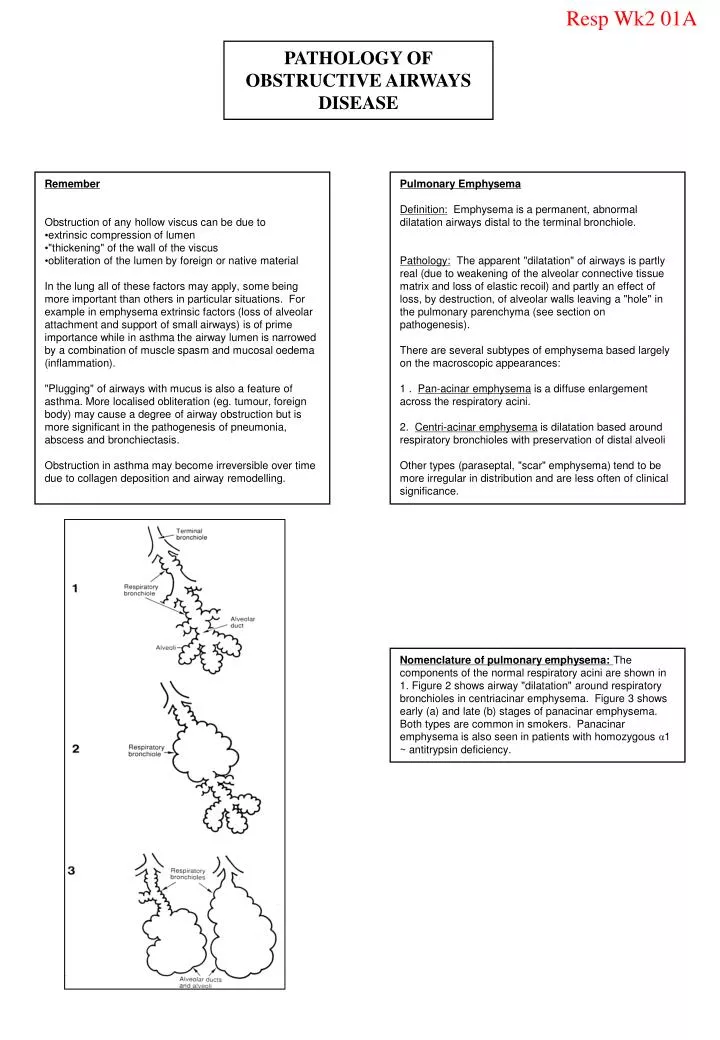
Resp Wk2 01A. PATHOLOGY OF OBSTRUCTIVE AIRWAYS DISEASE. Remember Obstruction of any hollow viscus can be due to extrinsic compression of lumen "thickening" of the wall of the viscus obliteration of the lumen by foreign or native material

E N D
Resp Wk2 01A PATHOLOGY OF OBSTRUCTIVE AIRWAYS DISEASE • Remember • Obstruction of any hollow viscus can be due to • extrinsic compression of lumen • "thickening" of the wall of the viscus • obliteration of the lumen by foreign or native material • In the lung all ofthese factors may apply, some being more important than others in particular situations. For example in emphysema extrinsic factors (loss of alveolar attachment and support of small airways) is of prime importance while in asthma the airway lumen is narrowed by a combination of muscle spasm and mucosal oedema (inflammation). • "Plugging" of airways with mucus is alsoa feature of asthma. More localised obliteration (eg. tumour, foreign body) may cause a degree of airway obstruction but is more significant in the pathogenesis of pneumonia, abscess and bronchiectasis. • Obstruction in asthma may become irreversible over time due to collagen deposition and airway remodelling. Pulmonary Emphysema Definition: Emphysema is a permanent, abnormal dilatation airways distal to the terminal bronchiole. Pathology: The apparent "dilatation" of airways is partly real (due to weakening of the alveolar connective tissue matrix and loss ofelastic recoil) and partly an effect of loss,by destruction, of alveolar walls leaving a "hole" in the pulmonary parenchyma (see section on pathogenesis). There are several subtypes of emphysema based largely on the macroscopic appearances: 1 . Pan-acinar emphysema is a diffuse enlargement across the respiratory acini. 2. Centri-acinar emphysema is dilatation based around respiratory bronchioles with preservation of distal alveoli Other types (paraseptal, "scar" emphysema) tend to be more irregular in distribution and are less often ofclinical significance. Nomenclature of pulmonary emphysema: The components ofthe normal respiratory aciniare shown in 1. Figure 2 shows airway "dilatation" around respiratory bronchioles in centriacinar emphysema. Figure 3 shows early (a) and late (b) stages of panacinar emphysema. Both types are common in smokers. Panacinar emphysema is also seen in patients with homozygous α1 ~ antitrypsin deficiency.
Resp Wk2 01B Macroscopic Features of Emphysema • Identify Figures A, B and C below as: • normal lung • centriacinar emphysema • panacinar emphysema A B C
Resp Wk2 02A Bullous Emphysema Bullous emphysema is a descriptive term denoting very large subpleural air-filled sacs. These may occur in any ofthe recognised major types of emphysema or as an isolated phenomenon. In the latter situation they may be responsible for spontaneous pneumothorax in young people. Pathogenesis of Emphvsema : (see diagram) Emphysema is caused by destruction of alveolar walls. Experimental installation of proteolytic enzymes in animals leads to pulmonary emphysema. l antitrypsin (l AT) is one ofa series of protease inhibitors which can antagonise the effect of enzymes such as elastase. l AT deficiency is an autosomal recessive disorder in which this activity is deficient. These patients have less than 10% of normal antiprotease activity and develop emphysema. Heterozygates have intermediate levels and are at a high risk if they smoke. 1 AT deficiency is also associated with liver dysfunction and cirrhosis. Cigarette smoke leads to increased accumulation and degranulation of neutrophils and macrophages in the lung ( ↑elastase activity) and also to inhibition of l AT activity). The habit is thereby highly implicated in the causation of emphysema. PATHOGENESIS OF EMPHYSEMA Degradation of Alveolar Walls Loss of Elastic Recoil ELASTIN ELASTASE l ANTITRYPSIN (Neutrophils, macrophages) In normal subjects the "background" level of elastase activity is counteracted by l antitrypsin (AT). Elastin degradation may occur with increased phagocyte degranulation or decreased l AT activity. IMMUNOLOGICAL STIMULI TO ACUTE AND CHRONICINFLAMMANON IN BRONCHIAL ASTHMA T = T LYMPHOCYTE, B = B LYMPHOCYTE, MC = MAST CELL,EO = EOSINOPHIL , IL4,5 = INTERLEUKINS 4,5 It can be seen that antigen exposure may lead to degranulation of mast cells (histamine, prostaglandins). This may be responsible for immediate bronchial contraction and wheeze. The eosinophil secretes platelet activating factor (PAF) and specific products such as eosinophil basic protein which stimulate chronic inflammation, epithelial damage and bronchial hyper~responsiveness.
Resp Wk2 02B Pathogenesis of Bronchial Asthma Historically asthma has been associated with the concept of"bronchial hyper~responsiveness". It is now thought that this phenomenon is due largely to a chronic inflammatory response in the airways. Exacerbations of inflammation leading to clinical worsening of symptoms may be due to a variety of factors: Atopy (type I hypersensitivity) Drugs (eg. aspirin) Infection (virus) Exercise Immunological mechanisms are thought to be important in initiating and maintaining the inflammatory response. In some patients there is an obvious allergen (eg. house dust mite) ~ extrinsic asthma. In patients with "intrinsic" asthma there is no obvious allergen and atopy is not a feature. Immunological and inflammatory features are otherwise the same in these two groups. Pathology of asthma (a fatal case) These specimens are from an autopsy on a 53 year oldfemale, known asthmatic Figure 1 Macroscopic specimen of lung showing oedematous narrowing of bronchi (large arrow). You will also see mucus plugging of airways (small arrow). Figure 2 Closer view showing extensive mucus plugging. Figure 3 Photomicrography showing a marked inflammatory response in an airway wall. Note shedding of damaged epithelial cells into mucus plug and subepithelial fibrosis.
Resp Wk2 03A Pathology of Emphysema Macroscopic appearance of an emphysematous lung Gross appearance of effects of cigarette smoke Ciliary damage – secondary to smoking Scanning electron micrograph of emphysema
Resp Wk2 03B Aetiology of airway obstruction in COPD Loss of support Mucosal Swelling Mucus in Irregular lumen Muscle spasm Pathogenesis of ObstructiveAirways Disease
Resp Wk2 03-D Comparison ofAsthma and COPD
Resp Wk2 04A Bronchitis andEmphysema Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease • Clinical features : • Chronic symptoms – not episodic • Smoking history • Non – atopic • Progressive breathlessness • Frequent infective exacerbations • Signs : • Tachypnoea • Hyperexpanded chest • Prolonged expiration • Pursed lip breathing • Quiet breath sounds Pink Puffer Blue Bloater What are the clinical features of Pink Puffers and Blue Bloaters?
Resp Wk2 04B Cor Pulmonale Accelerated Loss of Lung Function Due to Smoking (Green line) Effects of Stopping Smoking on Lung Function (Yellow and Blue lines) IT’S NEVER TOO LATE TO STOP SMOKING