Download
1 / 1
30 likes | 302 Views
B – Serum Immunofixation (Left) C – Urine Immunofixation (Below). A. Beginning of Chemo. Stem Cell Transplant. Diagnosis. Restaging. End of Chemo. Group B Streptococcal Septic Shock – A remarkable Case of Multiple Myeloma

E N D
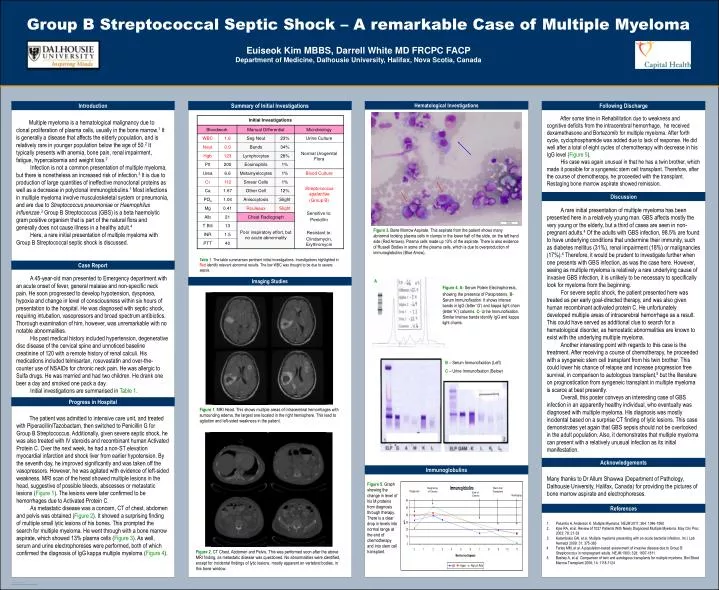
B – Serum Immunofixation (Left) C – Urine Immunofixation (Below) A Beginning of Chemo Stem Cell Transplant Diagnosis Restaging End of Chemo Group B Streptococcal Septic Shock – A remarkable Case of Multiple Myeloma Euiseok Kim MBBS, Darrell White MD FRCPC FACPDepartment of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada Introduction Summary of Initial Investigations Hematological Investigations Following Discharge After some time in Rehabilitation due to weakness and cognitive deficits from the intracerebral hemorrhage, he received dexamethasone and Bortezomib for multiple myeloma. After forth cycle, cyclophosphamide was added due to lack of response. He did well after a total of eight cycles of chemotherapy with decrease in his IgG level (Figure 5). His case was again unusual in that he has a twin brother, which made it possible for a syngeneic stem cell transplant. Therefore, after the course of chemotherapy, he proceeded with the transplant. Restaging bone marrow aspirate showed remission. Multiple myeloma is a hematological malignancy due to clonal proliferation of plasma cells, usually in the bone marrow.1 It is generally a disease that affects the elderly population, and is relatively rare in younger population below the age of 50.2 It typically presents with anemia, bone pain, renal impairment, fatigue, hypercalcemia and weight loss.2 Infection is not a common presentation of multiple myeloma, but there is nonetheless an increased risk of infection.3 It is due to production of large quantities of ineffective monoclonal proteins as well as a decrease in polyclonal immunoglobulins.1 Most infections in multiple myeloma involve musculoskeletal system or pneumonia, and are due to Streptococcus pneumoniae or Haemophilus influenzae.3 Group B Streptococcus (GBS) is a beta haemolytic gram positive organism that is part of the natural flora and generally does not cause illness in a healthy adult.4 Here, a rare initial presentation of multiple myeloma with Group B Streptococcal septic shock is discussed. Discussion A rare initial presentation of multiple myeloma has been presented here in a relatively young man. GBS affects mostly the very young or the elderly, but a third of cases are seen in non-pregnant adults.4Of the adults with GBS infection, 98.5% are found to have underlying conditions that undermine their immunity, such as diabetes mellitus (31%), renal impairment (18%) or malignancies (17%).4 Therefore, it would be prudent to investigate further when one presents with GBS infection, as was the case here. However, seeing as multiple myeloma is relatively a rare underlying cause of invasive GBS infection, it is unlikely to be necessary to specifically look for myeloma from the beginning. For severe septic shock, the patient presented here was treated as per early goal-directed therapy, and was also given human recombinant activated protein C. He unfortunately developed multiple areas of intracerebral hemorrhage as a result. This could have served as additional clue to search for a hematological disorder, as hemostatic abnormalities are known to exist with the underlying multiple myeloma. Another interesting point with regards to this case is the treatment. After receiving a course of chemotherapy, he proceeded with a syngeneic stem cell transplant from his twin brother. This could lower his chance of relapse and increase progression free survival, in comparison to autologous transplant,5 but the literature on prognostication from syngeneic transplant in multiple myeloma is scarce at best presently. Overall, this poster conveys an interesting case of GBS infection in an apparently healthy individual, who eventually was diagnosed with multiple myeloma. His diagnosis was mostly incidental based on a surprise CT finding of lytic lesions. This case demonstrates yet again that GBS sepsis should not be overlooked in the adult population. Also, it demonstrates that multiple myeloma can present with a relatively unusual infection as its initial manifestation. Figure 3. Bone Marrow Aspirate. This aspirate from the patient shows many abnormal looking plasma cells in clumps in the lower half of the slide, on the left hand side (Red Arrows). Plasma cells made up 13% of the aspirate. There is also evidence of Russell Bodies in some of the plasma cells, which is due to overproduction of immunoglobulins (Blue Arrow). Table 1. The table summarises pertinent initial investigations. Investigations highlighted in Red identify relevant abnormal results. The low WBC was thought to be due to severe sepsis. Case Report A 45-year-old man presented to Emergency department with an acute onset of fever, general malaise and non-specific neck pain. He soon progressed to develop hypotension, dyspnoea, hypoxia and change in level of consciousness within six hours of presentation to the hospital. He was diagnosed with septic shock, requiring intubation, vasopressors and broad spectrum antibiotics. Thorough examination of him, however, was unremarkable with no notable abnormalities. His past medical history included hypertension, degenerative disc disease of the cervical spine and unnoticed baseline creatinine of 120 with a remote history of renal calculi. His medications included telmisartan, rosuvastatin and over-the-counter use of NSAIDs for chronic neck pain. He was allergic to Sulfa drugs. He was married and had two children. He drank one beer a day and smoked one pack a day. Initial investigations are summarised in Table 1. Imaging Studies Figure 4. A- Serum Potein Electrophoresis, showing the presence of Paraproteins.B- Serum Immunofixation. It shows intense bands in IgG (letter ‘G’) and kappa light chain (letter ‘K’) columns. C- Urine Immunofixation. Similar intense bands identify IgG and kappa light chains. Progress in Hospital Figure 1. MRI Head. This shows multiple areas of intracerebral hemorrhages with surrounding edema, the largest one located in the right hemisphere. This lead to agitation and left-sided weakness in the patient. The patient was admitted to intensive care unit, and treated with Piperacillin/Tazobactam, then switched to Penicillin G for Group B Streptococcus. Additionally, given severe septic shock, he was also treated with IV steroids and recombinant human Activated Protein C. Over the next week, he had a non-ST elevation myocardial infarction and shock liver from earlier hypotension. By the seventh day, he improved significantly and was taken off the vasopressors. However, he was agitated with evidence of left-sided weakness. MRI scan of the head showed multiple lesions in the head, suggestive of possible bleeds, abscesses or metastatic lesions (Figure 1). The lesions were later confirmed to be hemorrhages due to Activated Protein C. As metastatic disease was a concern, CT of chest, abdomen and pelvis was obtained (Figure 2). It showed a surprising finding of multiple small lytic lesions of his bones. This prompted the search for multiple myeloma. He went through with a bone marrow aspirate, which showed 13% plasma cells (Figure 3). As well, serum and urine electrophoreses were performed, both of which confirmed the diagnosis of IgG kappa multiple myeloma (Figure 4). Acknowledgements Immunoglobulins Many thanks to Dr Allum Shawwa (Department of Pathology, Dalhousie University, Halifax, Canada) for providing the pictures of bone marrow aspirate and electrophoreses. Figure 5. Graph showing the change in level of his M proteins from diagnosis through therapy. There is a clear drop in levels into normal range at the end of chemotherapy and into stem cell transplant. References • Palumbo A, Anderson K. Multiple Myeloma. NEJM 2011; 364: 1046-1060 • Kyle RA, et al. Review of 1027 Patients With Newly Diagnosed Multiple Myeloma. May Clin Proc 2003; 78: 21-33 • Kalambokis GN, et al. Multiple myeloma presenting with an acute bacterial infection. Int J Lab Hematol 2009; 31: 375-383 • Farley MM, et al. A population-based assessment of invasive disease due to Group B Streptococcus in nonpregnant adults. NEJM 1993; 328: 1807-1811 • Bashey A, et al. Comparison of twin and autologous transplants for multiple myeloma. Biol Blood Marrow Transplant 2008; 14: 1118-1124 Figure 2. CT Chest, Abdomen and Pelvis. This was performed soon after the above MRI finding, as metastatic disease was questioned. No abnormalities were identified, except for incidental findings of lytic lesions, mostly apparent on vertebral bodies, in this bone window.