Download
1 / 45
450 likes | 487 Views
Explore the benefits, feasibility, and potential risks of laparoscopic surgery for ovarian cancer. Learn about primary, secondary, and debulking procedures, as well as restaging and upstaging considerations. Discover key findings and recommendations from comparative and meta-analysis studies in the field of gynecologic oncology.

E N D
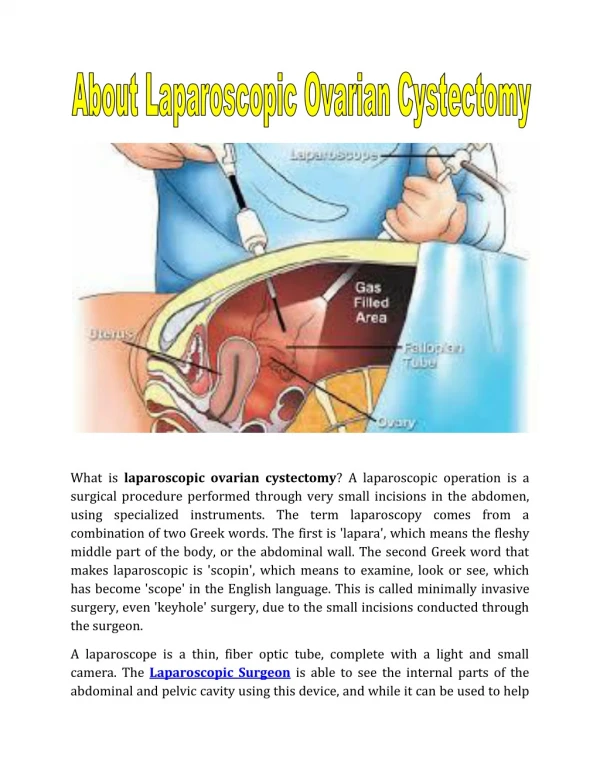
Laparoscopic Surgical Management of Epithelial Ovarian Cancer Cagatay Taskiran, MD, Assoc. Prof.VKV American Hospital, Division of Gynecologic Oncology
Primary trt for early stage disease Restaging Primary cytored’n for advanced disease Surgical trt for recurrent disease To assess resectability: Neoadjuvant CT VATS L/S & EOC
Standard Surgery for Early Stage Ovarian Cancer • Comprehensive surgical staging Exploration - Cytology and biopsies Hyst-BSO- fertility sparing surgery PPLND- Total Omentectomy Appendectomy
Up-staging Schuler et al, 1999, EJOGRB 401 patients, 24% up-staging • Diaphragma • Omentum • PPALN • Cytology
Literature Early stage ovarian cancer & Laparoscopy • Retrospective series • Case-control studies • Meta-analysis • Cochrane review
Literature Early stage ovarian cancer & Laparoscopy 1994, Querleu-Leblanc 9 patients • Still small series, number low • 11 studies, 9-42 pt, 88 multicenter • Approximately 400 patients
Comparative Studies & Feasibility Chi, AJOG, 2005, 50 pt LN number, omental size: no problem No conversion to L/T Survival rates similar Park, Ann Surg Oncol, 2008, 36 pt LN number, omental size: no problem Upstaging rate is same No recurrence within 20 months
Benefits of Laparoscopy Endometrial cancer – randomized studies EBL lower Shorter hospital stay Fewer postoperative complications Improved QOL Faster return to normal function Similar for ovarian cancer – no RCT, shorter interval to adjuvant chemotherapy
Benefits of Laparoscopy Ghezzi, 2 012, 88 pt Blood tx rate 2.8% vs 19.2% Postoperative complications 3.2% vs 31% Febrile morbidity Ileus Wound dehiscence Wound infection
Potential Benefits & Some Conflicts Cost Complications Hospital stay Performance – return to work – CT ?? Improved fecundity after fertility sparing surgery - adhesions
Possible Risks & Rupture Rupture – IC – Chemo – survival is worsened • L/T 10% and L/S 15-20% • Size and endobag usage • Rupture vs puncture ??
Meta-Analysis & Accepted 4 April AJOG 11 studies EBL lower Upstaging rate 23% Conversion to L/T 3.7% Recurrence rate 9.9% (6.7-14) Intraop rupture 25% !!!!! Only 1 port site-metastasis
Data Overall 12 hasta Borderline 8 pt EOC 4 pt (all restaging) LN number 31-84 Omentectomy no problem No conversion No intra-postop comp Median time 5 hr
Transperitoneal LA & Learning curve • >20 cases PLN number satisfactory, time shorter, complications decrease; LN number: 17-22 • Paraaortic LN number increase by years: 6----19 Kohler, GO, 2004
Transperitoneal LA & Duration Kohler, GO, 2004
Re-staging & Up-staging 14 studies 1971-1994
Timing of Restaging Lehner 1998 max. 15 days Kinderman 1996 max. 8 days Adequate staging is very important
Fanning, 2011, GO CT: omental metastasis – ascites 25 cases – 2 conversions: severe omental-RS 36% no residual Hospiatal stay median 1 day Blood loss 340 ml Median OS: 3.5 years Primary Debulking for Advanced Disease
Nezhat, JSLS, 2010 28 pt, 11 open after diagnostic L/S %88 optimal Time and complication rates are same Blood loss and hospital stay less 9 NED, 6 AWD, 2 DOD Primary Debulking for Advanced Disease
Magrina, 2013, GO, 2006-2010 L/S: 9, Robot:10, L/T:33 patients 15 types of different procedures No conversion No difference: Op. Time, comp’n, complete debulking, survival Endoscopy: Blood loss and hospital stay L/T: 3 major procedures, upper and lower quadrants Secondary Cytoreduction
Nezhat, JSLS, 2012, only L/S 1999-2009, secondary 20, tertiary 3 cases %82 optimal 200 min, 75 ml, stay 2 days 1 conversion No intraop complication NED:12 AWD:6 DOD:4 Median DFS: 72 months Secondary Cytoreduction
There is limited data on the role laprascopicsurgeryforearlystageovariancancer Although it wasstarted at nearlythesame time periodswith EC and CC it was not populirezed Itseemsfeasibleforsurgicalprocedures, upstagingrates, adequacy of lymphadenectomyandomentectomy Survivalratesaresimilarwithlaparotomy Port site metastasis is rare, Major problem is tumorrupture Conclusion
There is limited data on thevalue of laparoscopicsurgeryforrecurrentdisease. Itseemsfeasibleforhighlyselectedpatients at veryexperiencedcenters Itmay be goodwaytoassessresectabilityforadvancedcasesbothbeforeprimarysurgeryandafter NACT VATS should be performedforpatientshavingmoderateto severe pleuraleffusionbeforreabdominalcytoreduction Conclusion