Download
1 / 15
150 likes | 315 Views
ITU Workshop on “ E-health services in low-resource settings: Requirements and ITU role ” (Tokyo, Japan, 4-5 February 2013). Abu Dhabi Weqaya Programme Tackling NCDs: Application to Low and Middle Income Health Markets. Reehan Sheikh Technology Strategist Platform Health

E N D
ITU Workshop on “E-health services in low-resource settings: Requirements and ITU role” (Tokyo, Japan, 4-5 February 2013) Abu Dhabi Weqaya Programme Tackling NCDs: Application to Low and Middle Income Health Markets Reehan Sheikh Technology Strategist Platform Health reehan.sheikh@opensecurehealth.com
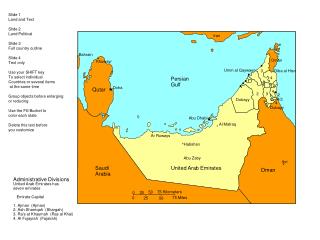
Abu Dhabi has been ideal market for innovation in health data 2.1m lives: “Big enough to matter, small enough to manage…” Highly strategic government with broad-based popular trust Extreme pace and depth of socio-economic development – very high burden of NCDs Plural and diverse payers and providers Relatively well-resourced health system enabling innovation
Abu Dhabi’s greatest health challenge Implementing the Dubai declaration GCC Council of Ministers UAE: World’s 2nd highest prevalence of diabetes Addresses at least six of the eight objectives
Modeling suggests rapid cost increase Direct healthcare cost Societal cost Predicted costs of UAE National diabetes treatment, AED
Delivering model at scale: Overview of Weqaya • Approach • Screen Screen individuals iteratively • 97% adult Emiratis screened (>190,000) • Plan Clinical Standards, website/call centre • Act Clinical care, targeted lifestyle behaviour change (diet, physical exercise, tobacco) 1 PLAN SCREEN ACT • Interventions • Population • Standard clinical care • Nutrition (trans-fats, food labeling) • Physical activity (gyms, AD UPC) • Tobacco control • Group • Workplaces and schools • Local communities, families • Segments: Disease groups e.g. diabetics • Individual • Clinical care • Encourage: Weqaya reports • Enable: Website/call centre 2 Population Group Individual
An individual score and customized call to action • Principles of data feedback • Patients should have access to their own health data: • Personal Health Record (secure paper mail-out) • Electronic Health Record (www.weqaya.ae) • Smart Portable Health Record (Weqaya Data Architecture)
Pay for Quality and Pay for Health Pay for Quality • Based on compliance with evidence-based care pathways and clinical quality indicators • Mechanism set-out in Standard Contract (between Healthcare Facilities and Health Insurers) • Expectation it will affect base payment by <10% • “Compliance with high quality care receives a bonus” • Based on individual health status • Health initially defined as 10-year risk of cardiovascular event (heart attack or stroke) • Contract between individual and Disease Management Programme • AED1,000 per 1% reduction in risk to maximum of AED5,000 (5%) • “No health improvement – no money” Pay for Health
In AD eHealth systems are a platform for health Everyone can know their numbers… … and the numbers can change health outcomes % engaged with care* % with HbA1c <7.5% % with LDL:HDL ratio <3.5 Control Weqaya Control Weqaya Control Weqaya 2008 2009 2010
Two domains of Weqaya action • Healthcare Sector • Clinical care standards • Patient empowerment • Customer-centred services • Research and Innovation • Health Guardians • Nutrition • Physical activity • Tobacco control • Alcohol control • Employers and schools • Urban Planning 9
We set clear targets based on global evidence Annual Weqaya targets Target risk reduction
Screening: Adaptations for medium and low income countries $1 Per person cost Adaptation $2 • Non-clinical staff • Train the trainer • SMS-based reporting $15 • Clinical/para-clinical staff • Train the trainer • SMS-based reporting • Personal Health Record
Data Exchange in low and medium income countries A B C • Data capture (mobile device) • Unique identifier (patient, clinician, etc.) • (Simplified) diagnosis, treatment provided, outcome, etc. • Standardised data • Kilobyte range (works with 2G mobile phone) • Data store • Donors • Clinicians • Programme managers • Academia • WHO • UN – Development Goals (MDGs) Option to create “central health philanthropy bank” to administrate
Range of data systems enable secure ubiquity • Opt-out screening • Opt-in data sharing Measuring health • Ubiquitous Weqaya Programme • Point of decision prompts (e.g. Weqaya label on healthy food) • At home monitoring • Secure data sharing Taking health promoting action
Standardized and Centralized Health Data 1 Health & Wellness data can be capture in the field using basic mobile technologies 2 3 All Health & Wellness information is saved centrally for population and individual level analysis Healthcare workers can immediately access data captured in the field and begin a two-way dialog 4 Personal health/wellness tracking and intervention can be tied to clinical information allowing a view into effectiveness of intervention and patient behaviour change 5 In healthcare facilities, providers can get a full view of the patient
Thank You Questions? Reehan Sheikh Platform Health reehan.sheikh@opensecurehealth.com www.opensecurehealth.com