Download
1 / 13
170 likes | 676 Views
Motor System I: Pyramidal Tract . Objectives . Introduction Origin of the Pyramidal Tract Effects of Stimulation of the Cerebral Cortex Course and Termination Effects of Lesions and Clinical Correlation Corticobulbar Fibers and Effects of Interrupting Them.

E N D
Introduction Origin of the Pyramidal Tract Effects of Stimulation of the Cerebral Cortex Course and Termination Effects of Lesions and Clinical Correlation Corticobulbar Fibers and Effects of Interrupting Them Motor System I: The Pyramidal Tract
I. Introduction • Pyramidal Tract (PT) in pyramid of medulla (hence its name). • Consists of two tracts: 1) Corticospinal and 2) Corticobulbar (reflecting whether the fibers terminate in the spinal cord or brainstem. • Fibers of 1 and 2 terminate on sensory neurons, interneurons and motorneurons. • PT provides the central control for initiating the skilled motor movements. • PT also has effects on myotatic reflexes, muscle tone and cutaneous reflexes. • Phylogenetically it is new. • Ontogenetically, its myelination is not completed until the 2nd year postnatally.
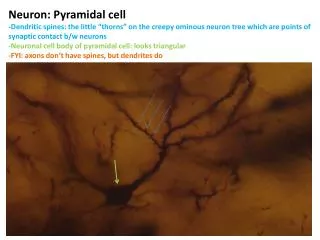
II. Origin (see Fig 1) • Pyramidal cells in layer V of cerebral cortex (“new” or neocortex has 6 layers). • 20-24% PT fibers originate from Brodmann’s area 4 (primary motor cortex). 3-4% of these come from giant pyramidal (Betz) cells. • 30% from areas 3, 1 and 2 (primary sensory cortex). • 30% from area 6 (includes PMA and SMA). • 15% from areas 5 and 7 (sup. parietal lobule).
III. Effects of Stimulation of the Motor Cortex (Fig. 1) • Stimulation evokes discrete, isolated movements on the opposite body side. • Contraction of specific muscles always related to site of stimulation on area 4. From this, the concept of a “motor homunculus” has emerged. • Stimulation of area 4 causes flick-like flexions or extensions involving few muscles. • Stimulation of area 6 or other areas may result in patterned movements involving many muscles. • Area 4 does not plan or initiate movements but organizes the spatial and temporal patterns of muscle contractions during movements. • Planning of the movement probably occurs in SMA which is part of area 6.
IV. Course and Termination (Figs. 2-5) • PT fibers leave the cortex, pass in the ipsilateral corona radiata, internal capsule and cerebral peduncle where they are arranged somatotopically. • Same fibers then enter the basilar pons where they are arranged in bundles, after which these bundles coalesce at the medulla level where they form the medullary pyramid. • PT fibers terminating at the level of the brainstem are, for the most part, corticobulbar fibers. Collaterals of PT fibers also terminate in the basal ganglia, thalamus, red nucleus and reticular formation. • At the medulla/spinal cord transition, 75-90% of the PT fibers cross the midline and descend in the lateral funiculus as the lateral corticospinal tract. • The uncrossed 10-25% descends in the anterior funiculus as the anterior corticospinal tract. These fibers, however, cross the midline at their spinal level of termination. • Lat. corticospinal tract fibers are distributed: 55% to cervical, 20% to thoracic and 25% to lumbosacral spinal levels. Ant. corticospinal fibers terminate at cervical and upper thoracic spinal levels. • Most corticospinal fibers terminate in the intermediate gray matter (Rexed’s laminae IV to VIII. A few terminate in lamina IX. • Facilitation bias exists towards flexor motor neurons innervating the upper limb and extensor motor neurons for the lower limb. After PT lesions those muscles will be affected more severely than their antagonists.
V. Effects of Lesions and Clinical Correlation • Experimental medullary PT lesion causes permanent loss of contralateral discrete digital movements, loss of abdominal and cremasteric reflexes and lasting hypotonia (flaccid muscles). • Clinical PT lesion result in the “PT syndrome” with spastic paralysis and augmented DTR’s (deep tendon reflexes), loss of abdominal and cremasteric reflexes and abnormal plantar (i.e., Babinski) reflex. “Clasp knife” phenomenon can be elicited on the paralyzed upper limb. • 5-10 hrs after lesion onset, the Babinski sign can be elicited. Paralyzed muscles become progressively spastic a few days after onset. While digital movements are permanently lost, some movement returns to the proximal limbs. • Spasticity results from hyperinnervation of spinal motor neurons by surviving fibers (both sensory and other motor).
VI. Corticobulbar Fibers and Effects of Interrupting Them (Fig. 5) • Corticobulbar fibers are PT fibers that terminate in brainstem sensory relay nuclei, reticular formation and some cranial nerve motor nuclei (motor V, motor VII, ambiguus, hypoglossal motor and spinal accessory – XI). • Oculomotor, trochlear and abducens motor nuclei do not receive PT fibers. • Corticobulbar fibers on one side of the brain are distributed bilaterally to much of the above nuclei, except that V and XII receive more crossed than uncrossed PT fibers. • Corticobulbar innervation of motor VII is as follow: 1) dorsal ½ of VII receives bilateral innervation; 2) ventral ½ of VII is innervated only by the contralateral corticobulbar fibers. • Unilateral lesions of the corticobulbar tract results in transient, mild deviation of the jaw and tongue to the contralateral side of the lesion. However a permanent paralysis on the lower face will be observed (patient cannot smile or show you his/her teeth). • Bilateral lesions of the corticobulbar tracts results in pseudobulbar palsy (inability to chew, speak, swallow and breath).