Download
1 / 46
460 likes | 612 Views
Anemia – What do you mean it’s not IMHA???. Jason M. Eberhardt DVM, MS, DACVIM. Overview. One of the most common CBC abnormalities 10-30% of patients Why is it still so confusing? Back to basics Systematic approach to anemia Avoiding common pitfalls. Some thoughts….

E N D
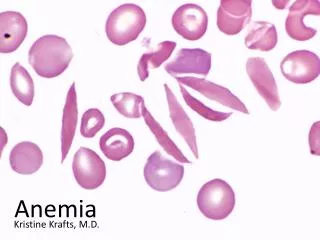
Anemia – What do you mean it’s not IMHA??? Jason M. Eberhardt DVM, MS, DACVIM
Overview • One of the most common CBC abnormalities • 10-30% of patients • Why is it still so confusing? • Back to basics • Systematic approach to anemia • Avoiding common pitfalls
Some thoughts… • “You need to have the correct diagnosis before you can recommend the correct treatment.” • “If you always have the correct diagnosis then you’re not a really veterinarian…you’re probably a breeder.” • “You need to run a minimum of 5 diagnostic tests prior to starting steroids…”
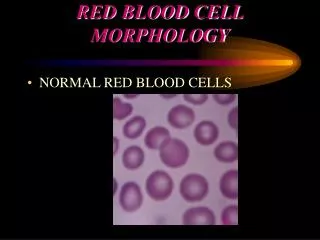
Definitions • Mean Corpuscular Volume (MCV) – Avg. RBC size • Macrocytosis • Microcytosis • Normocytic • Mean corpuscular Hgb concentration (MCHC) – [ ] of Hgb vol. RBC • Hypochromic • Normochromic • Macrochromic • Reticulocytes – Immature RBCs released from B.M. early • Normoblasts/metarubricytes – nucleated erythrocytes
Definitions continued… • Poikilocytosis – Variation of RBC shape • Rouleaux – Stacks of coins • Small amount is normal • Increased fibrinogen or acute phase proteins • Typically seen in inflammatory conditions • Autoagglutination – Aggregate in grapelike clusters • Must be differentiated from rouleaux • Rouleaux disperses when blood is mixed with saline
Rouleaux or Autoagglutination Rouleaux Autoagglutination
Before I go any further… • Where do I start……. • Back to basics!!!
The first step… • Remember the Total Protein!!! • It’s the other half of “blood” • It’s cheap! • It’s fast • DO NOT OVERLOOK! • Are just the RBCs being affected or the plasma as well?
The next steps… • Morphologic classification • RBC indices • Bone marrow response • Regenerative vs. Non-regenerative • Description of poikilocytosis? • Macrocytic, hypochromic, regenerative anemia with marked spherocytosis
Morphological classification • Usage of RBC indices (MCV/MCHC) to “describe” the RBCs. • Remember MCV/MCHC are MEAN calculations • Large # of RBCs affected prior to increases/decreases • Allows characterization of anemia into a category • Helps with ranking differential diagnoses • Are found on nearly all in-house CBC units
Normocytic normochromic • Most common • “Normal” RBCs • Most commonly denotes a non-regenerative anemia • Usually lacks RBC morphology changes • “Pre-regenerative” • First 1-3 days of acute loss/lysis
Macrocytic hypochromic • Usually indicates a regenerative anemia • Reticulocytes are relatively larger then mature RBCs • Hypochromic because Hgb synthesis is not complete • Only 8% of 6752 patients with reg. anemia had both increased MCV & decreased MCHC DiNicola et al.
Macrocytic normochromic • Usually misclassification due to insensitivity of MCV/MCHC • Autoagglutination? • Feline Leukemia • Poodles – Congenital dyserythropoiesis • Notanemic • Large problem in humans • B12 &/or folate deficiency • Role in veterinary medicine is questionable
Microcytic hypochromic • Consistent with an iron deficiency anemia • Inadequate amount of Hgb is produced • Typically seen in chronic conditions • GI blood loss • Severe parasitism • PSS & Hepatic atrophy • Myelodysplastic syndromes • Congenital: Akitas, Shiba Inu, Chow breeds • Not typically hypochromic
Bone marrow response • Is there a regenerative response? • Evaluation of reticulocytosis • No reticulocytosis/polychromasia expected during first 1-3 days (maybe not at all if anemia stays mild) • Response peaks 4-5 days (with normal B.M.) • Erythrocyte indices start to change 7-14 days
What is consider regenerative??? • Normal patient should have <45,000-60,000 absolute retic count • Absolute counts • 60,000-150,000 Early/mild response • 150,000-250,000 Mild-moderate • >250,000-500,000 Moderate-Marked • Relative % • 1-4 % - Mild • 5-20 % - Moderate • > 20 % - Marked
Regenerative anemia • Loss vs. Lysis • LOOK AT TOTAL PROTEIN!!!! • External blood loss • Low to low-normal T.P. • Hemolytic disease • High to high-normal T.P.
Acute external blood loss • PCV does not fully reflect severity first 1-3 days • Reticulocytosis should start by day 3 • Peak reticulocytes day 4-7 • PCV increases to low normal w/in 2 wks • May take up to 4-5 weeks to return to normal • Mild anemia does not stimulate strong erythropoietin release
Chronic blood loss • Iron deficiency and negative protein balance develops after “several” weeks in adults • Occurs more rapidly in young animals (low iron stores) • Initially non/”pre” regenerative • Period of regenerative anemia depending on severity • Eventually returns to being poorly/non-regenerative • Often have thrombocytosis • Remember RBC indices do not change for 7-14 days • Getting blood transfusions???
Hemolytic anemia • Hemolysis is a mechanism NOT a “disease” • Lots of “non” immune mediated causes • Low serum phosphorus • Normal to increased T.P. • Spherocytosis and/or autoagglutination • Over interpretation is common • Can be seen in diseases that are not “primary” • Positive Coomb’s Test?
Direct Coomb’s Test • Identifies presence antibodies/compliment on RBCs • They may/may not actually be directed towards RBCs • This may/may not actually cause damage to RBCs • Neither highly specific or sensitive for IMHA • Positive in 60-70% of cases • Positive results – should have other evidence of IMHA • Effect of steroids? • **NOTE** – What is the end point of the test?????
Breaking it down… • Try to subclassifyinto intravascular vs. extravascular • Alters differential diagnosis • Intravascular – Rapid breakdown in vascular system • Pink urine, pink serum • Hemoglobinuria best indicator • Hyperbilirubinemia typically more profound then in extravascular • Extravascular – removal of RBCs by spleen, liver, B.M. • More common • Often has icterus, splenomegaly, hepatomegaly
Immune mediated • “Immune-mediated” is a mechanism NOT a disease. • Can be 2nd to a number of possible causes • Infectious – Babesiosis, Ehrlichiosis, Leishmaniasis, Rickettsioses, Mycoplasma haemofelis, FeLV • Neoplasia • Drugs • Can be initially non-regenerative (esp. in cats)
“Penny” 6 year FS Cocker • Presented for severe lethargy, “yellow skin” and “peeing blood” • Severe, macrocytic, normochromic strongly regenerative anemia with mild-moderate spherocytosis • Slide agglutination negative • High total protein • Abdominal ultrasound WNL • Infectious disease titers all negative
The “Penny” dilemma • Needed multiple transfusion in a 5-6 day period • Continued to have hemolysis despite aggressive immunosuppressive therapy • Where do we go from here??? • “Peeing” blood – hemoglobinuria • Intravascular hemolysis
Intravascular hemolysis • Immune mediated • Phosphofructokinase deficiency • Eng. Springers, Amer. Cockers • Babesiainfection • Snake envenomation • Heavy metal to toxicity • Zinc • Copper
“Penny” 6 yrFS Cocker Spaniel • Presented for severe lethargy, yellow skin and “peeing blood” • Severe, macrocytic, normochromic strongly regenerative anemia with mild-moderate spherocytes • Abdominal ultrasound WNL • Infectious disease titers all negative
“Sheldon” 9 yr MC Jack Russell • Presented with clinical evidence of anemia • Severe leukocytosis (54,000), severe anemia (9%), high normal platelets, mild-moderate reticulocytosis • Total Protein – 4.9 g/dL • VF, Ehr. Neg.
IHMA??? • Started on prednisone, cyclosporine, doxycycline • Needed 2nd transfusion 1 week later • Added azathioprine • PCV still low 2 weeks later • Chest rads and abd. u/s WNL • Increased prednisone, continued on cyclosporine and azathioprine • 3rd transfusion in 4 weeks • Added leflunomide • Repeat abdominal ultrasound WNL
More anemia!!! • Initial PCV/TP at EAC • 12%/4.8 • Reference lab work • Hypoalbuminemia (2.6 g/dL), globulin WNL (1.7 g/dL), BUN increased (mild), Total bilirubin (mild) • Inflammatory leukogram • Severe reticulocytosis
What’s going on??? • Horrible IMHA??? • Another type of hemolytic anemia? • GI bleeding (from prednisone?, GI mass?) • Diagnostic plan??????????? • Explain the decreased total protein
Non-regenerative anemia • Very common!!! • Usually normocytic normochromic • Microcytic, hypochromic anemias • Usually no poikilocytosis • Huge majority are mild-moderate in severity • 2nd to systemic disease
Before going any further… • Is neutropenia and/or thrombocytopenia also present? • What is the duration of clinical signs? • How severe are the clinical signs?
I need more RBCs… • Mild-moderate NR anemia • Search for an underlying disease first • Anemia of chronic/inflammatory disease • Neoplasia, renal disease, hepatic disease, infectious, inflammatory, endocrine • Drugs
Severe non-regenerative anemia • Toxicity • Estrogen? • Drugs • Renal disease • More than just decreased erythropoietin • Chronic dz, decr. RBC lifespan, ineffective production, blood loss
Why can’t it be easy??? • Bone marrow exam • Took a long time to develop • Can take even longer to resolve • Can still be very confusing and frustrating
Bone Marrow disease • Immune mediated • Maturation arrest vs. Pure Red Cell Aplasia • Myelophthisic syndromes - multiple cell lines often affected • Aplastic anemia – B.M. replaced by fat • Can be 2nd to chronic ehrlichiosis • Myelofibrosis– B.M. replaced by fibrous • Myelonecrosis – Drugs, toxins, viral • Neoplasia
“Howard” 9 yr MN DSH • Progressive lethargy, wt. loss for severalweeks • Marked (12%), macrocytic, normochromic anemia • Total protein 6.2 g/dL • Absolute reticulocyte count 40,000 • Retic. total 2% • Corrected 0.65% • FelV/FIV negative • Chest radiographs, abdominal ultrasound WNL
Why cats are not small dogs… • 50% of cats with immune mediated disease initially had a non-regenerative response Kohn et al. 2006 • 2/3 were <3 years (range was 1-9 yr) • Bone marrow disease – 53% • Infectious – 22% • Hemolysis – 11% • Immune Mediated – 6% • Severity of anemia associated with B.M. disease Korman et al. 2013
Bone marrow or bust • Owner noticed gradual decline • More consistent with non-regenerative disease • Transfusion • Recheck 2-3 days later vs. bone marrow now • Marked erythroid hypoplasia/aplasia • Immune mediated vs. FelV • Bone marrow IFA positive for FelVStutzer et al. 2010
RBC shape descriptions • Many have little/no clinical significance • Anisocytosis, elliptocytes, codocytes, leptocytes, *echinocytes* • Spherocytes – Evidence of hemolysis • Acanthocytes - Hemangiosarcoma, hepatic dz • Schistocytes - DIC, Fe def, CHF, myelofibrosis, hemangiosarcoma, other neoplasia
Summary • Anemia is a common abnormality • Cause can often be elusive • Vital to approach systematically • RBC indices, bone marrow response, poikilocytosis • DON’T FORGET THE TOTAL PROTEIN!!!