Download
1 / 41
430 likes | 1.47k Views
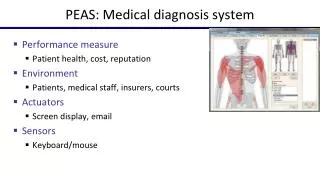
TIME CRITICAL DIAGNOSIS SYSTEM in MISSOURI. Meeting Purpose. Why Time Critical Diagnosis Matters STEMI, Stroke, Trauma Patient Care The Trauma System Model Implementation: Progress and Goals Missouri Regulations Next Steps.

E N D
Meeting Purpose • Why Time Critical Diagnosis Matters • STEMI, Stroke, Trauma Patient Care • The Trauma System Model • Implementation: Progress and Goals • Missouri Regulations • Next Steps
Why Time Critical Diagnosis System Matters:Leading causes of death in Missouri 1stHeart Disease, including ST-Elevation Myocardial Infarction (STEMI) 3rd Stroke 4th Trauma-injury-accidents, motor vehicle accidents, suicide, homicide, other; Leading cause of YPLL
TCD Project History 2003 – Missouri Foundation for Health (MFH) identified the need for EMS/Trauma Reform 2005 – Dr. Bill Jermyn accepts State EMS Medical Director Position 2006 – Emergency Medical Care System planning ‘07-08+ – TCD Task Forces (Stroke/STEMI and Trauma) 2008 – Authorizing Legislation 2008+ –Time Critical Diagnosis stroke and STEMI implementation teams 2009 – ACS COT Review 2010 –NHTSA Review
TCD System Goal Improve health outcomes for Missourians who suffer acute trauma, stroke or STEMI by establishing a Time Critical Diagnosis (TCD) System. Prompt treatment reduces death and disability.
Why Time Critical Diagnosis Matters Prompt treatment reduces death and disability. HEART DISEASE • Outcomes for heart attack victims can be improved with an integrated care delivery system. • STEMI, ST-Segment Elevation Myocardial Infarction, is a common form of heart attack that is time critical.
Why Time Critical Diagnosis Matters Prompt treatment reduces death and disability. STEMI • Shorter time from door-to-balloon (PCI) - lower risk of mortality • Moving towards first medical contact to balloon • Symptom onset to treatment time greater than 4 hours independent predictor of one-year mortality • Faster treatment and lower in-hospital mortality associated with hospital “specialization” and emphasis on PCI as principal mode of reperfusion
Why Time Critical Diagnosis Matters Prompt treatment reduces death and disability. STROKE • Missouri-ranks 7th in stroke prevalence • Missouri’s stroke death rate – 11% higher than national rate • 15-30% will be disabled (leading cause of disability) • 20% require institutionalization first 3 months post-stroke
Why Time Critical Diagnosis Matters Prompt treatment reduces death and disability. STROKE • t-PA Treatment within 180 minutes from symptom onset: • Better odds of improvement at 24 hours • Improved 3-month outcome • Patients treated after 180 minutes • Poorer outcomes • More hemorrhages
Why Time Critical Diagnosis Matters Prompt treatment reduces death and disability. TRAUMA • Missouri death rates for unintentional injuries increased 25% between 1991 and 2006 • Missouri death rates for accidental injuries, suicides, falls and MVC’s exceed national rates • There are gaps, particularly in rural areas, for timely access to trauma care
Why Time Critical Diagnosis Matters • Current protocol – unlike trauma, ambulances triage to the nearest hospital for stroke or STEMI, not necessarily a facility equipped to deliver necessary level of care for stroke or STEMI • Patients who self-transport may not have the knowledge to go to the right facility • Rural populations face unique challenges in access to timely care
Why Time Critical Diagnosis Matters That’s the problem. What’s the solution?
Creating a Time Critical Diagnosis System • The Solution: • The Right Care • at the • The Right Place • in the • The Right Time
Creating a Time Critical Diagnosis System • The solution: • Using the Trauma System • as a Model
Using Trauma System as a Model Trauma System: • Improves Patient Outcomes and Saves Lives • 50% reduction in preventable death rate after implementation • Decrease in cases of sub-optimal care from 32% to 3% • Improves Hospital Outcomes • Better outcomes compared to voluntary system • Cost Savings through more efficient use of resources • Improves Regional Outcomes • Regional system accommodates regional and local variations
Implementation: Progress and Goals Guidelines for the most appropriate care.
Implementation: Progress and Goals Legislative Synopsis: 2008: House Bill 1790 enabling reform passed unanimously by the Missouri Assembly and signed into law RSMo 190-100 Definitions RSMo 190.200 Public Information & Education RSMo 190.241 Center Designation RSMo 190.243 Transportation to Centers
Implementation: Progress and Goals Developing the System: August 2008: TCD Stroke/STEMITask Force compiled formal recommendations Sept.’08-Present: TCD Trauma Task Force convened and compiling recommendations 2008-Present: Stroke and STEMI Implementation groups meeting regularly and compiling standards for stroke and STEMI center designation and EMS
Missouri Regulations • Law authorizes DHSS to promulgate regulations • Inclusive process for drafting regulations • DHSS submits as “Proposed Rules” • Office of the Secretary of State and • Joint Committee on Administrative Rules • Public Comment Period • Final Rules
Missouri RegulationsBoth Stroke & STEMI Four Levels of Center Designation Level I Functions as resource center within region Level II Provide care to high volumes of stroke and STEMI patients Level III Access into system in non-metropolitan areas, more limited resources and generally refer to higher level center Level IV Access in rural areas, stabilize and prepare for rapid transfer to higher level of care
Missouri Regulations Both Stroke & STEMI • Voluntary process • Stroke/STEMI Program-24/7 (all levels) • Medical Director • Program Manager/Coordinator • Staff meet and maintain core requirements to provide care • One-call activation protocol • Transfer – network agreements
Missouri Regulations Both Stroke & STEMI • Data submission for statewide registry • Performance improvement and patient safety requirements • Public education to promote prevention and signs and symptoms awareness
Missouri RegulationsRegional Plans Regional or community based plans for transporting trauma, STEMI or stroke patients may be submitted to DHSS. 190.200 RSMo but not required
Missouri Regulations Next Steps • Finish Community-Based Plan • Conduct legal and administrative reviews • Submit proposed stroke and STEMI regulations to Secretary of State’s office in 2010; Trauma regulations to follow in 2011 • Allow public comment period (at least 30 days) • Compile public comment response (90 days) • File with JCAR (30 days) • File final order of rulemaking, effective 30 days after published
Next Steps Public Education • Work group compiling plan • Launch public education campaign • TCD System • Signs and symptoms and importance of calling 911
Next Steps Professional Education • Professional education planning (Fall-2009 through Spring-2010) • Conduct professional education (Begin Summer 2010)
Next StepsTracking Progress Create evaluation mechanism to track progress and outcomes
Next Steps Quality Assurance • Review existing data system • CDC Info Aid • MU Health Informatics • Convene quality assurance work group • Define data points (benchmarks, PI, indicators, outcomes) • Review existing systems for collection • Compile plan to populate state Stroke and STEMI registry without creating burden for reporters • Implement plan • Update state database and reporting methodologies • Training • Compile reports to support PI/Quality Assurance • Regional Processes
Next Steps Center Application • DHSS creates application—filed as part of regulations • Once regulations effective, hospitals may submit application (similar to trauma center application and review process currently in place) • DHSS conducts review • DHSS approves designation for those that meet standards