Download
1 / 29
290 likes | 567 Views
Depression in children. Dr.Ksh. Chourjit Singh Prof. of Pediatrics Regional Institute of Medical Sciences, Imphal National Chairperson, Growth & Development Chapter, IAP National Executive Board Member Advisor HIV/AIDS in Children Task Force, Manipur State. Past President, East Zone, IAP

E N D
Depression in children Dr.Ksh. Chourjit Singh Prof. of Pediatrics Regional Institute of Medical Sciences, Imphal National Chairperson, Growth & Development Chapter, IAP National Executive Board Member Advisor HIV/AIDS in Children Task Force, Manipur State. Past President, East Zone, IAP President, NNF, Manipur State Branch
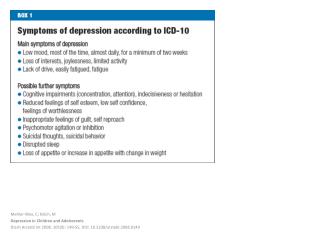
Introduction • Depression in school-age children and adolescents remain a long-overlooked Health problem • As prevalent as in adults • Common cold of mental illness – Clinical Depression • Specially in childhood – is a major health problem
Severity of Problem • 5% children at any given time • 1% of Pre-school children • 2% of school-age children • 5% of adolescents are affected • 25-50% of all children & adolescents in Psychiatric treatment are for depression & its related problems • More common in boys than girls – 5:1 school-age children • Adolescent girls than boys - 2:1
Severity of Problem …. Untreated Depression can be taken as important cause of suicide in adolescents, even adults
Why depression in young ? A) Risk factors • Children referred to mental health providers for school problems • Children with medical problems • Asthma • Diabetes • Epilepsy • Many chronic childhood diseases
Why depression in young ? ……. • Law and order problems • Frequent bandh/ strikes • Frequent school closures • Ethnic group clashes • Insecure feelings • Conflict environment • Watching television a lot i.e. more than 6 hours a day
Risk factors ….. • Rural vrs Urban children • Sexually harassed children • Children with family history of depression • Genetically potential • What is happening in an individual child’s life
B) Why depression runs in families • Genetics • Even if a child never contacts with depressed parents, child may also likely to be depressed • Marital difficulties • Broken family/ marital problems • Divorce plus depression in parents • Parenting problems • Hard to be good parent when depressed • Parenting problems whether from parents or from child
C) Can experience depression at any age – Presentation? • Shortly after birth & very young • Failure to thrive • Disrupted attachments to others • Developmental delays • Social withdrawal • Separation anxiety • Sleeping and eating problems
C) Chance of depression at any age… • Between 6-12 years of age • Fatigue • Sadness • Inability to feel pleasure • Irritability & Insomnia • Lack of self esteem • Stomach ache and headache
C) Chance of depression at any age… • Hallucinations • Agitation & extreme fears • Weight changes • Difficulty with school work • Apathy • Lack of Motivation • Social withdrawal
C) Chance of depression at any age… • Adolescent • Over-sleeping • Socially isolated • Acting out in self destructive ways • Sense of hopelessness • Despairing thoughts • Weight changes
Future of depressed school-age children • If untreated in time – affects the children • School performance and learning • Social interaction and development of normal peer relationships • Self-esteem and life skill acquisition • Parent-child relationship & sense of bonding
Future of depressed school-age children…. • Lack of trust – can lead to Substance abuse • Disruptive behaviour • Violence and Aggression • Legal troubles and even suicide Depression thinking can become part of a child’s developing personality, leaving long-term effects in place for the rest of the child’s life.
Behavioural changes – What? • Professional attention decreases • Classroom disruption • Expulsion from school • School failure • Injury to themselves or others • Symptoms ADHD • Truancy • Delinquency
Stress in students leading to depression • Parental pressure to perform and to stand out among other children • If not come up to expectations • Frustration • Physical stress • Aggression • Undesirable complexes
Stress in students leading to depression… Under-Performers • Negative traits • Shyness • Unfriendliness • Jealousy • World to loner
Over-scheduling a student’s life • Non-availability of time for extra-curricular activities after school • No proper place for ventilation & breathing space • Unwanted learning like music, painting or outstanding in sports • Too many crammed schedule & unmindful of the children’s choice • Unadjusted school systems and tremendous amount of homework – spending their evenings, weekends and vacations
Over-scheduling a student’s life… • Loss of interest in studies • Under-perform due to excess academic pressure Students often carry enormous amount of anxiety and negative personal traits & massive attention problems • Non-effortless learning • Physio-Psychological transition of students • Mainly affected elementary to Junior High School
Diagnostic Points • Transient depression or sadness • Impairment in child’s ability to function • Two types • Dysthymic disorder • Major depressions • Dysthymic disorder – less severe but lasts longer • Chronic depression/Irritability > 1 year
Diagnostic Points …. • Onset about 7 years of age • 2-6 symptoms within 5 years • Leads to major depression/ Double depression • Untreated Dysthymic disorder will experience Remission within 6 years • Prevalence of depression increases with age – 5 percent of all teens
What can be done • Diagnostic evaluation – success to treatment • All disorders be discovered and addressed • Medication • Mood stabilisers • Anti-anxiety • Anti-depressants • Stimulants
What can be done…Individual therapy • Often beneficial for patients & specially help with issues • Family conflicts • Self-esteem • Relaxation strategies • Mood and anger control • Better communication
School environment • Interaction • School Counsellor • Principal • Psychologist • Teachers and Parents • Psycho-educational treatment • Speech and occupational therapy
School environment… • Counselling • Curriculum modification • Resource classes • Behavioural modification system • Self-contained classrooms
Home/ Parental environment • Family and Home modification\ • Homely life environment
Family therapy • Defining Family members role and responsibility • Better communication & behavioural Reward systems
Don’t overload your child with too many after-school activities and responsibilities. Let children learn to pace themselves. Don’t enrol them in every class along and don’t expect them to be first in everything.