Download
1 / 17
170 likes | 277 Views
CARDIOVASCULAR AUTONOMIC NEUROPATHY IN DIABETICS. Michelle Anderton MVS 442 February 4, 1999. BASIC DEFINITIONS.

E N D
CARDIOVASCULAR AUTONOMIC NEUROPATHY IN DIABETICS Michelle Anderton MVS 442 February 4, 1999
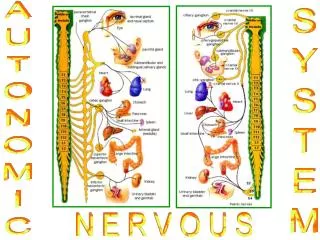
BASIC DEFINITIONS Autonomic Nervous System: Part of the nervous system that is responsible for control and regulation of the involuntary bodily functions, including those of the heart, blood vessels, visceral smooth muscles and glands. It consists of the sympathetic system, which in general stimulates the body to prepare for physical action and emergency, and the parasympathetic system which stimulates the opposite responses. Neuropathy: Any disease of the nervous system
ABOUT AUTONOMIC NEUROPATHY • It is difficult to diagnose due to: • diffuse organ involvement • gradual onset
ABOUT AUTONOMIC NEUROPATHY • AN can affect: • ocular pupil • sweat glands • GI tract • bladder • sex organs • adrenal medullary system • cardiovascular system
ABOUT AUTONOMIC NEUROPATHY • It is a common complication of both types of diabetes mellitus (type I and II) • One of the earliest detectable complications of long-term glucotoxicity
ABOUT AUTONOMIC NEUROPATHY (POSSIBLE CAUSES) • Excess of sorbitol (a crystalline alcohol) in the nerve tissue • interferes with normal nerve function via an osmotic effect that results in nerve swelling • also leads to decreases in nerve myoinositol which is important for normal operation of the Na+ - K+ - AT-Pase pump • important in maintaining proper membrane potential • a decrease in pump activity = decrease in nerve conduction velocity
WHAT IS CARDIOVASCULAR AUTONOMIC NEUROPATHY?? • It is basically cardiac denervation which can result in: • a fixed HR that is unresponsive to exercise or stress, which in turn can lead to: • cardiac arrhythmias and sudden death • there is an increased risk when under anesthesia and for the occurrence of silent myocardial infarction and myocardial ischemia (lack of blood supply to the heart muscle).
WHAT IS CARDIOVASCULAR AUTONOMIC NEUROPATHY?? • Difficult to detect: • need to rule out various other disorders that have similar symptoms to CAN such as: • vestibular problems, hypoglycemia, dehydration. adrenal insufficiency, anemia and hypothyroidism
CAN EXERCISE ACTUALLY REDUCE CARDIOVASCULAR AUTONOMIC NEUROPATHY IN DIABETICS??
PURPOSE AND SUBJECTS • Purpose of study: • compare cardiovascular response to exercise in patients with non-insulin-dependent diabetes mellitus (NIDDM) with a group of healthy subjects • 108 NIDDM subjects • 112 healthy subjects
PROCEDURE • each group was matched to one another according to age, sex, physical fitness and presence of hypertension • groups were given clinical exams to determine weight, height, BMI and BP • all patients performed two cardiovascular tests: deep breathing and lying to standing. • tests were scored on a basis of a set normality • normal = 0 , abnormal = 2
PROCEDURE • then an overall cardiac autonomic nervous function (CAN) score was given • then a cycle ergometer test was administered until either max. HR or exhaustion occurred
FINDINGS • during exercise, SBP and DBP changes were much lower in the diabetic patients • during recovery HR decrease was also significantly slower • even diabetic subjects without outward signs of CAN experienced the above results • no differences in total work capacity and peak HR were found
CONCLUSIONS • there is an abnormal CV response during exercise in NIDDM patients, which could be due to: • “depressed contractility or reduction in preload, possibly due to decreased ventricular compliance”
CONCLUSIONS • “autonomic dysfunction may directly affect left ventricular function...abnormal coordination of the peripheral vasculature could impair ventricular preload and afterload, thus changing ventricular volume and reducing pressure and ejection fraction response during exercise”
LIMITATIONS • the fact that this was an isolated test doesn’t quite tell us how the heart would react to a prolonged exercise program. • it is possible that with the proper routine, the heart could be trained to function at a higher level
PREVENTION • maintenance of a normal or near-normal blood glucose level could help prevent, or at least slow the accumulation of sorbitol, which could reduce the affects of CAN