Download
1 / 36
520 likes | 966 Views
POLYCYSTIC OVARIAN SYNDROME (PCOS). TL KHUMALO 30 AUGUST 2018. Dr TL Khumalo hails from Durban, KwaZulu-Natal, currently practicing as a Specialist Obstetrician and Gynaecologist in Edendale Regional Hospital (Pietermaritzburg )

E N D
POLYCYSTIC OVARIANSYNDROME (PCOS) TL KHUMALO 30 AUGUST 2018
Dr TL Khumalo hails from Durban, KwaZulu-Natal, currently practicing as a Specialist Obstetrician and Gynaecologist in Edendale Regional Hospital (Pietermaritzburg) • She obtained her undergraduate degree at the Nelson R. Mandela School of Medicine and obtained her Fellowship in Obstetrics and Gynaecology via the University of KwaZulu-Natal in 2016 • She has keen interests in seeing both Maternal health and the stigmatized Disorders of Sex development improve • She has research interests in Infertility management in low resource settings • Her research interests are in the field of Sexual Reproductive Health
DISCLOSURES • NIL DISCLOSURES
OUTLINE • BACKGROUND • DEFINITION / PREVALENCE • ISSUES RELATED TO PCOS • APPROACH TO MANAGEMENT
SYNDROME Greek Etymology Sun ~ TOGETHER DRAMEIN ~ TO RUN SYNDROME SunDRAMEIN ~ TO RUN TOGETHER
BACKGROUND • 1935 : Stein IF and Leventhal ML designated PCO as a syndrome • ’80s/’90s : Addition of ultrasound criteria • 2003 : Rotterdam Consensus Conference • 2018 : International evidence-based guideline for the assessment and management of polycystic ovary syndrome 2018
BACKGROUND • : International evidence-based guideline for the assessment and management of polycystic ovary syndrome 2018 • Over 3 000 delegates SUPPORT OPTIMAL PATIENT CARE AIMS PROVIDE CLEAR INFORMATION ASSIST CLINICAL DECISION MAKING
BACKGROUND • Ovarian Theca Cells >> Under the control of LH/IGF-1 >> Produces Testosterone >> Granulosa cells convert (Aromatase enzyme) to active Oestradiol • Increasedandrogenproduction • Increased free androgens
CONTROVERSIES • Rotterdam criteria is over 10yrs old • Serum AMH is under intense debate • Misnomer of the term poly“cystic” which is referring to aarested follicles not cysts • COCP and the WHO MEC (2015) • Ethics of Distributive Justice
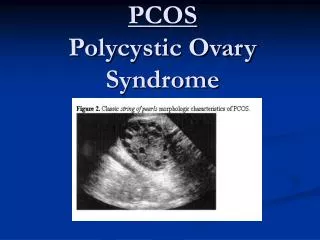
PCOS OA ~ Oligo-Anovulation HA ~ Hyper-androgenism PCOM ~ Polycystic Ovarian Morphology
OA:Oligo-Anovulation • Primary / Secondary Amenorrhoea • Oligomenorrhoea • Less than 8 episodes of menses a year • Cycle length exceeding 35 days (n:21-35) • Complications PCOM diagnosis on US > No longer recommended in the presence OA
OA:Oligo-Anovulation Mx AIM • Balance the steroid hormones (ER/PR) Compete with Oestrogen at receptor level /Hypothalamic level Block conversion to active hormone – Inhibit Aromatase enzyme Anti-androgenic / Anti-oestrogenic action Anti-oestrogenic action
OA:Oligo-Anovulation Mx • Increase SHBG • Suppress of FSH/LH > Negative Feedback on the axis • Reduction in free circulating Androgens • Regulation of menses > Risk reduction of endometrial hyperplasia / EC Low dose COCP
OA:Oligo-Anovulation Mx Low dose COCP • 35mcg Ethinyloestradiol + Cyproterone Acetate not for 1st line in PCOS • Consider combining with Metformin in Adolescents or BMI ≥ 25kg/m² • Regulation of menses > Risk reduction of endometrial hyperplasia / EC
HA: Hyperandrogenism Biochemical FSH:LH Ratio Testosterone DHEAS AMH Clinical Hirsutism Acne Alopecia Virilisation • Grade the Hirsutism > modified Ferriman-Gallwey score • Mx: Block the peripheral action of hair follicle 5α Reductase > Testosterone to Di-hydrotestosterone therefore blocked
HA: Hyperandrogenism Mx • Grade the Hirsutism > modified Ferriman-Gallwey score (1961) • Rx: Block the peripheral action of hair follicle 5α Reductase > Testosterone to Di-hydrotestosterone therefore blocked • Lifestyle modification • COCP +Drosperinone / Desogestrel / Norgestimate • Anti-androgens : • Spironolactone 50-200mg / day • Cyproterone Acetate 50-100mg (5-15days Induction / Maintenance) • *Ensure adequate contraception / Prevent under virilisation of the male foetus*
HA: Hyperandrogenism Mx • Insulin Lowering / Increase Insulin Sensitisation • Generally off-label / EBM practice • Under the control of LH/IGF-1 : Ovarian Theca Cells produce Testosterone • Adjunctive BMI ≥ 25kg/m² for Ovulation induction • Metformin 500mg tds > Slow release preferred • Reduces Hepatic Glucose production / Lowering Insulin levels • Possible improvement in Ovarian Steroidogenesis
HA: Hyperandrogenism Mx • GnRHa • Blockade of GnRH > Blockade of FSH / LH • Zoladex 3.6mg s/c (3-6 months) • Leuprolide 3.75mg imi (3-6 months) • Add-back therapy if intolerable side-effects • 25-30mcg transdermal Oestradiol • Tibolone is great for oestrogen withdrawal • S/E: Hot flashes, Reduce Bone mineral density, Atrophic vaginitis, FSD
HA: Hyperandrogenism Mx Anti-androgens + COCPs if no control of HA > 6mo
PCOM: Polycystic Morphology • Challenge is not so much the size or volume • US has poor sensitivity in the background of OA /HA • Arrest of Pre-antral follicles • Failure of LH surge • Leading to failure of Ovulation
MULTI-DISCIPLINARY TEAM Gynaecologist Dietician Physician/Endocrinologist Fertility Specialist Support Groups
Mx of PCOS Dietician • Lifestyle modification • Moderate exercise (30 minutes /week) • Target to normalize BMI • Reduction of adipose tissue > Reduces peripheral sites for Androgen production • Higher spontaneous pregnancy rates with lifestyle adjustments
Mx of PCOS Physician/Endocrinologist • Metabolic control • IGT / Insulin Resistance • Risk of Metabolic syndrome secondary to Obesity • Higher incidence of Depressive / Anxiety Disorders
Mx of PCOS Gynaecologist Fertility Specialist • OVULATION INDUCTION AGENTS • Letrozole • Clomiphene Citrate (CC) 50mg / 100mg /150mg • CC + Metformin
OVULATION INDUCTION • OVULATION INDUCTION AGENTS • Letrozole • Clomiphene Citrate • CC + Metformin • LETROZOLE • Aromatase inhibition • Anti-oestrogenic > Reduction up to 98% in Oestrogen levels • FDA approved for HR+ Breast cancer • Competitively blocks production by binding to the haeme of its CP450 unit • Does not reduce production of mineralo-corticosteroids • 2.5mg/dusual dosage • Doses exceeding 2.5mg/d may cause reduced libido
OVULATION INDUCTION • OVULATION INDUCTION AGENTS • Letrozole • Clomiphene Citrate • CC + Metformin • Clomiphene Citrate • Mechanism of stimulating ovulation remains elusive • Anti-oestrogenic properties • Competes with Oestrogen binding sites • Increase in FSH / LH • Pre-ovulatory LH surge / Corpus luteum maturation • 50mg / 100mg / 150mg • Half-life: 5 – 7 days • Time to peak: 4 – 10 days • Average 7 days
OVULATION INDUCTION • OVULATION INDUCTION AGENTS • Clomiphene Citrate
Mx of PCOS Support Groups www.pcosaa.org #PCOSsupport