Download
1 / 1
10 likes | 126 Views
Changes in PrP genotype, clinical signs and PrP res deposition through the time-course of a scrapie epidemic. K. M. McIntyre † , S. Gubbins † , A. Chong ‡ , N. Hunter ‡ , M.B. Gravenor § , E. Stevenson † , W. Goldmann ‡ , J. Dale † and M. Baylis †.

E N D
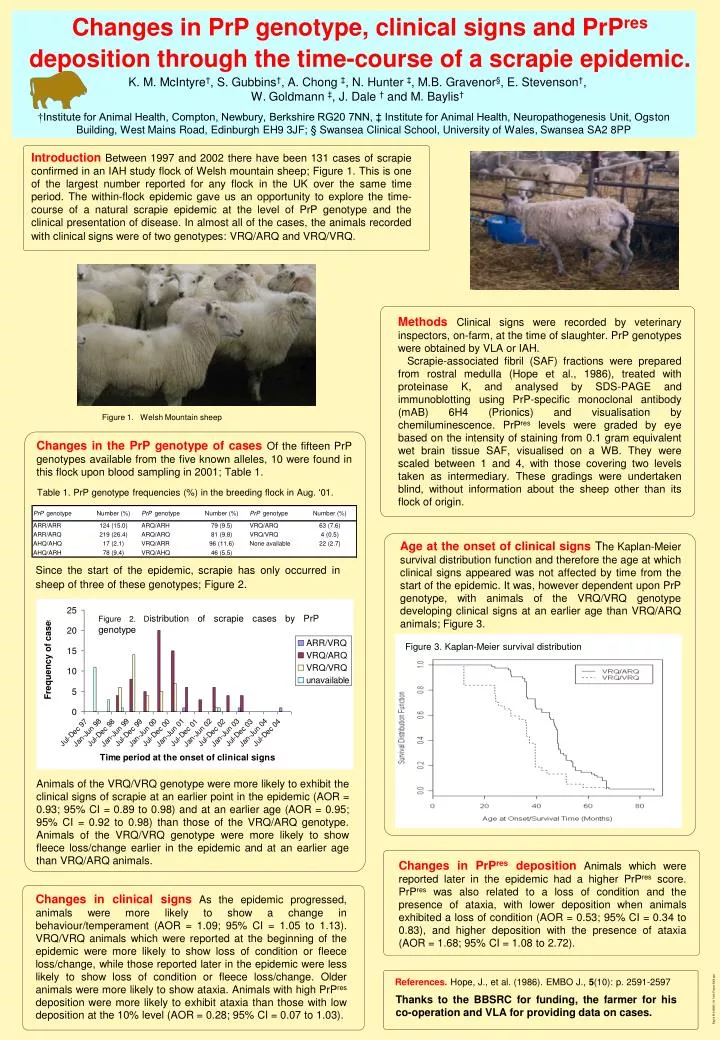
Changes in PrP genotype, clinical signs and PrPres deposition through the time-course of a scrapie epidemic. K. M. McIntyre†, S. Gubbins†, A. Chong ‡, N. Hunter ‡, M.B. Gravenor§, E. Stevenson†, W. Goldmann ‡, J. Dale † and M. Baylis† †Institute for Animal Health, Compton, Newbury, Berkshire RG20 7NN, ‡ Institute for Animal Health, Neuropathogenesis Unit, Ogston Building, West Mains Road, Edinburgh EH9 3JF; § Swansea Clinical School, University of Wales, Swansea SA2 8PP Introduction Between 1997 and 2002 there have been 131 cases of scrapie confirmed in an IAH study flock of Welsh mountain sheep; Figure 1. This is one of the largest number reported for any flock in the UK over the same time period. The within-flock epidemic gave us an opportunity to explore the time-course of a natural scrapie epidemic at the level of PrP genotype and the clinical presentation of disease. In almost all of the cases, the animals recorded with clinical signs were of two genotypes: VRQ/ARQ and VRQ/VRQ. MethodsClinical signs were recorded by veterinary inspectors, on-farm, at the time of slaughter. PrP genotypes were obtained by VLA or IAH. Scrapie-associated fibril (SAF) fractions were prepared from rostral medulla (Hope et al., 1986), treated with proteinase K, and analysed by SDS-PAGE and immunoblotting using PrP-specific monoclonal antibody (mAB) 6H4 (Prionics) and visualisation by chemiluminescence. PrPres levels were graded by eye based on the intensity of staining from 0.1 gram equivalent wet brain tissue SAF, visualised on a WB. They were scaled between 1 and 4, with those covering two levels taken as intermediary. These gradings were undertaken blind, without information about the sheep other than its flock of origin. Figure 1. Welsh Mountain sheep Changes in the PrP genotypeof casesOf the fifteen PrPgenotypes available from the five known alleles, 10 were found in this flock upon blood sampling in 2001; Table 1. Table 1. PrPgenotype frequencies (%) in the breeding flock in Aug. ‘01. Age at the onset of clinical signs The Kaplan-Meier survival distribution function and therefore the age at which clinical signs appeared was not affected by time from the start of the epidemic. It was, however dependent upon PrP genotype, with animals of the VRQ/VRQ genotype developing clinical signs at an earlier age than VRQ/ARQanimals; Figure 3. Since the start of the epidemic, scrapie has only occurred in sheep of three of these genotypes; Figure 2. Figure 2. Distribution of scrapie cases by PrP genotype Figure 3. Kaplan-Meier survival distribution Animals of the VRQ/VRQ genotype were more likely to exhibit the clinical signs of scrapie at an earlier point in the epidemic (AOR = 0.93; 95% CI = 0.89 to 0.98) and at an earlier age (AOR = 0.95; 95% CI = 0.92 to 0.98) than those of the VRQ/ARQ genotype. Animals of the VRQ/VRQ genotype were more likely to show fleece loss/change earlier in the epidemic and at an earlier age than VRQ/ARQ animals. Changes in PrPres depositionAnimals which were reported later in the epidemic had a higher PrPres score.PrPres was also related to a loss of condition and the presence of ataxia, with lower deposition when animals exhibited a loss of condition (AOR = 0.53; 95% CI = 0.34 to 0.83), and higher deposition with the presence of ataxia (AOR = 1.68; 95% CI = 1.08 to 2.72). Changes in clinical signsAs the epidemic progressed, animals were more likely to show a change in behaviour/temperament (AOR = 1.09; 95% CI = 1.05 to 1.13). VRQ/VRQ animals which were reported at the beginning of the epidemic were more likely to show loss of condition or fleece loss/change, while those reported later in the epidemic were less likely to show loss of condition or fleece loss/change. Older animals were more likely to show ataxia. Animals with high PrPres deposition were more likely to exhibit ataxia than those with low deposition at the 10% level (AOR = 0.28; 95% CI = 0.07 to 1.03). References. Hope, J., et al. (1986). EMBO J., 5(10): p. 2591-2597 Thanks to the BBSRC for funding, the farmer for his co-operation and VLA for providing data on cases. Baylis M 040820_04 York Poster 2004.ppt