Download
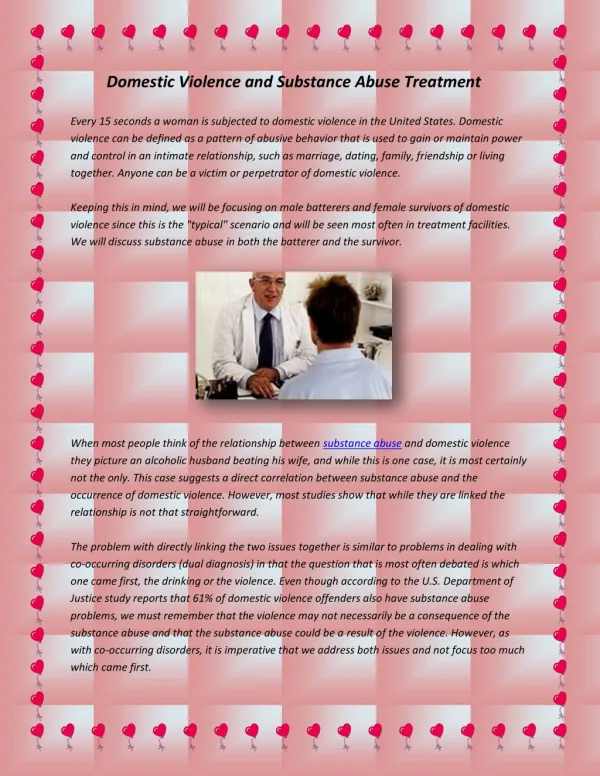
1 / 18
180 likes | 419 Views
Substance Abuse Treatment and Technology. Michael Vela LMSW Hickory Trail Hospital. Statistics. In 2008, an estimated 20.1 million Americans aged 12 or older were current (past month) illicit drug users. This estimate represents 8.0 percent of the population aged 12 or older.

E N D
Substance Abuse Treatment and Technology Michael Vela LMSW Hickory Trail Hospital
Statistics • In 2008, an estimated 20.1 million Americans aged 12 or older were current (past month) illicit drug users. This estimate represents 8.0 percent of the population aged 12 or older. • Illicit Drugs include: marijuana, cocaine, heroin, hallucinogens (LSD, mushrooms, Ecstasy, Ketamine, PCP), and inhalants; and the nonmedical use of prescription-type pain relievers, tranquilizers, stimulants, and sedatives. • In 2008, an estimated 22.2 million persons aged 12 or older were classified with substance dependence or abuse in the past year (8.9 percent of the population aged 12 or older). Of these, 3.1 million were classified with dependence on or abuse of both alcohol and illicit drugs, 3.9 million were dependent on or abused illicit drugs but not alcohol, and 15.2 million were dependent on or abused alcohol but not illicit drugs.
Statistics • Slightly more than half of Americans aged 12 or older reported being current drinkers of alcohol in the 2008 survey (51.6 percent). This translates to an estimated 129.0 million people, which is similar to the 2007 estimate of 126.8 million people (51.1 percent). • More than one fifth (23.3 percent) of persons aged 12 or older participated in binge drinking at least once in the 30 days prior to the survey in 2008. • In 2008, heavy drinking was reported by 6.9 percent of the population aged 12 or older, or 17.3 million people
Treatment Needs and Alcohol Reasons Percent Not Ready to Stop Using 42.0% Cost/Insurance Barriers 34.5% Social Stigma 18.8% Access 11.7% Did Not Think Needed Treatment Thought Could Handle without Treatment 11.6% Did Not Know Where to Go for Treatment 11.1% Did Not Have Time 4.1% Treatment Would Not Help 3.1% Other Barriers 3.1% In 2007, 7.8 percent of persons aged 12 or older (an estimated 19.3 million persons) needed treatment for an alcohol problem in the past year. Of the 19.3 million persons who needed alcohol treatment, 8.1 percent (1.6 million) received treatment at a specialty facility Nearly nine tenths (87.4 percent) of individuals who needed treatment neither received it nor perceived the need for it Only 4.5 percent perceived a need for treatment but did not receive
Principles for Effective Treatment • Addiction is a complex but treatable disease that affects brain function and behavior • No single treatment is appropriate for everyone • Treatment needs to be readily available 4. Effective treatment attends to the multiple needs of the individual • Remaining in treatment for an adequate period of time is critical • Counseling—individual and/or group—and other behavioral therapies are the most commonly used forms of drug abuse treatment
Principles for Effective Treatment 7. Medications are an important element of treatment for many patients, especially when combined with counseling and other behavioral therapies 8. An individual’s treatment and services plan must be assessed continually and modified as necessary to ensure treatment needs are met • Many drug-addicted individuals have other mental disorders 10. Medical detox. Is only the first stage of addiction treatment and by itself does little to change long term abuse 11. Treatment does not need to be voluntary to be effective • Drug use during treatment must be monitored continuously as lapses during treatment do occur • Treatment should assess presence of HIV, Hepatitis and other infectious disease as well as provide preventative measures to reduce high risk behavior
Treatment Options • 12 step recovery groups (not considered specialized treatment) • Out Patient Therapy, Out Patient Detoxification and Outpatient Psychiatry • Intensive Outpatient • Medically Assisted Detoxification • Inpatient Rehab • Residential Treatment • 12 step based • Medical/Social model • Who Provides Treatment? LCDC, LMSW, LPC, LPCI, LCSW, MD, Nurse Practitioner • What does Treatment involve?
Treatment • Most treatments are cognitive behaviorally based, individual and group • Focus on helping clients make changes in their life (stages of change, and motivational interviewing) • 12 step information • Medication? Source of controversy.
Treatment Outcomes • Long-term drug use results in significant changes in brain function that can persist long after the individual stops using drugs. • Because drug addiction is typically a chronic disorder characterized by occasional relapses, a short-term, one-time treatment is usually not sufficient. For many, treatment is a long-term process that involves multiple interventions and regular monitoring.
Treatment Outcomes • Relapse rates remain high with most patients having 2 treatment admissions per year (SAMHSA, 2001). Given the high rates of relapse, increasing prevalence rates, and mortality, new treatment approaches that address biological, psychosocial, and environmental factors need to be developed in order to increase abstinence rates and reduce relapse. (Bordnick et al. 2008)
Treatment and Technology • MRI, CT SCAN, and the brain • Scientists are able to look at the brain while clients’ cravings are triggered through image cues. Only fractions of a second are needed. • Medication is developed as a result to work by targeting specific neurotransmitters as well as receptors in the brain • Clients are now able to understand how drugs affect there brain, as well as why cravings can be so intense.
Virtual Reality Programming • Exposure therapy used to treat a wide variety of psychiatric disorders • Primarily a part of CBT • Virtual reality exposure therapy has been used to treat panic disorder, social phobia, fear of flying, fear of heights, and arachnophobia • Shows strong promise for PTSD with Iraq and Afghanistan war vets.
Rationale • Virtual reality incorporates a human-computer interaction • Provides active participation with a three-dimensional, multisensory virtual environment allowing the participant to derive a sense of presence in the virtual • For example, a person experiencing a swinging bridge over a cliff in virtual reality will often sway, and the VR elicits reactions (e.g., mild anxiety, vertigo) similar to how they would feel on a bridge in the real world.
VR and Substance Abuse • individuals with substance use disorders experience increases in craving and exhibit modest changes in autonomic responses, such heart rate and skin conductance, when exposed to drug-related versus neutral stimuli. • Cravings increased when participants were exposed to a virtual bar scene, a party, and a kitchen that contained alcohol. Cravings did not increase when participants were exposed to neutral stimuli.
Further Benefits • Real world stimuli vs. Safe place stimuli • When drug use measures are used in cue reactivity studies, the typical finding is a modest increase in drug-seeking or drug use behavior • VR may be an effective alternative to visualization or other methods of exposure. The stimuli are controlled, and thus the clinician can discuss specific cues or responses with the participant.
Conclusion • Comprehensive treatment is needed • Biopsychosocial needs must be taken into account in order to prevent/ decrease relapse rates as well as spiritual and physical. • Evidence based treatment is key • Treatment should be INDIVIDUALIZED!!!!
Resources Bordnick et al. (2008). Assessing reactivity to virtual reality alcohol based cues. Addictive Behaviors. 33. 743–756. Carter et al. (2008) Location and longing: The nicotine craving experience in virtual reality. Drug and Alcohol Dependence. 95. 73-80 Gorrindo, T. and Groves, J. E.. (2009). Computer Simulation and Virtual Reality in the Diagnosis and Treatment of Psychiatric Disorders. Academic Psychiatry. 33(5). 413-417. National Institute on Drug Abuse. (2009) Principles of Effective Drug Treatment: A research based guide. NIH Publication No. 09–4180 SAMSHA. (2009). National Survey on Drug Use and Health: Alcohol Treatment: Need, Utilization, and Barriers. http://oas.samhsa.gov/2k9/AlcTX/AlcTX.htm. U.S. Department of Health and Human Services (2008) National Survey on Drug Use and Health: National Findings. http://oas.samhsa.gov/nsduh/2k8nsduh/ 2k8Results.cfm#1.1
The End Hickory Trail Hospital Michael Vela LMSW 2000 Old Hickory Trail Hospital Desoto TX 75115 972-298-7323 Michael.vela@psysolutions.com