Download
1 / 125
1.25k likes | 1.42k Views
Addiction Medicine (ADM). Steven C. Boles, D.O ., FASAM Board Certified - FP ASAM Certified – ADM Board = American Osteopathic Board of Family Physicians ASAM = American Society of Addiction Medicine

E N D
Addiction Medicine (ADM) • Steven C. Boles, D.O., FASAM • Board Certified - FP • ASAM Certified – ADM • Board = American Osteopathic Board of Family Physicians • ASAM = American Society of Addiction Medicine • Adjunct Clinical Faculty - Midwestern University Arizona College of Osteopathic Medicine
Case #1: “Don’t drink before surgery….” • 45 y/o M, post-op ORIF femur fx • Becomes agitated, slightly febrile • Remains tachycardic, on POD#2 • His last drink was 3 DAYS AGO • He was given 4mg lorazepam initially in the ER, and some BZD’s during surgery 12 hrs later • He is given 80mgs Valium PO that day • But still pulls out his IV, wants to walk, and • Hears noises that aren’t there, per the RN.
Case #1: “Don’t drink before surgery….” • The pt at this point • has not had his risk for alcohol withdrawal syndrome (AWS) recognized • except possibly by the ER. • But that concern, Dx, and Rx • has not been followed-up on • during all the attention • given his surgical problem.
Case #1: “Don’t drink before surgery….” • The pt at this point has had • partial Rx for AWS, • blunting its development, • but NOT preventing • the progression into the emergence • of early delirium tremens.
Case #1: “Don’t drink before surgery….” • He hears noises that aren’t there, per RN. • He is given IV Haldol 5mgs q 4hrs x 2 • And calms down. • He receives Ativan & Haldol • Over the next 48 hrs, in decreasing taper • Goes home POD #5
Case #1: “….., but if you do, always tell your doctor” • REMEMBER : • Always give BZD’s BEFORE HALDOL • To avoid SZ’s • And if Haldol is given IV, • Extrapyramidal side effects (EPS’s) • Rarely, if ever, occur. • And what is the top dose of IV Haldol (haloperidol) that may be given to a human being???????
Case #1: Alcohol Withdrawal Syndrome (AWS) & Thiamine • Give thiamine 100mgs PO/IM/IV • BEFORE ANY GLUCOSE IV • To prevent precipitating : • - Wernicke’s encephalopathy • - Korsakoff’s confabulatory amnestic psychosis
Case #1: AWS & Thiamine • Give ALL pts at least 100 mg/day PO. • However, • If alcoholic encephalopathy is present : • - give 200 mg TID, either PO or IV • - for 4 WEEKS • And how would one quickly test for this type of encephalopathy?
CLINICALLY:Alcoholic Frontoparietal Hippocampal Encephalopathy • Detection : simply add a small test to the neuro exam • Give them a pen and paper, and ask them to, “Draw me a clock that says 10 after 11, please.” • Takes 2 minutes or less • You may be VERY surprised at the response from someone so talkative
Case #1: AWS & Thiamine • IF EITHER: • Wernicke’s encephalopathy, or • Korsakoff’s amnestic psychosis • are present: • give 1000mg/day of thiamine x 4 wks • (that’s not a misprint)
Case #2: “Lying to your doctor can be fatal” • 39 y/o F, (+)chronic pain, • Rx’d MTD (methadone) 40 mg/day, X 6 yrs, • presents for detox from BZD’s & cocaine (family angry w/her) • Wants to stay on her methadone (MTD) • States, “I was in jail for 3 days, • and all they gave me was Risperdal, • and now I’m starting to have WD”.
Case #2: “Lying to your doctor can be fatal” • So, pt started on detox for cocaine/BZD • And, she is given her usual • 40 mg MTD/day on day #1 of detox (20 mg BID) • On day #2, pt mildly sedated, • 3 hrs post 20mg AM MTD dose. • Total MTD = 60mg thus far • Prior to PM dose, pt is barely arousable (intoxicated), RR=6/min • Passed out, lying sideways, across her bed.
Case #2: “Lying to your doctor can be fatal” • What is the dose of methadone • that can fatal, • if given to an opioid naïve pt? • According to Goodman & Gilman’s • “The Pharmacological Basis of Therapeutics”, • (the King James’ version of pharmacology) • it’s only 60mg.
Case #2: “Lying to your doctor can be fatal” • Brother verifies she was in jail for 6 wks. • Given 12.5 mg naltrexone PO, • not naloxone (active by IV route). • Pt simply wakes up, has some coffee, • writes a letter (RR=22) and stays up all night. • Additional 62.5 mg naltrexone given over next 3 days (MTD obviously DC’d).
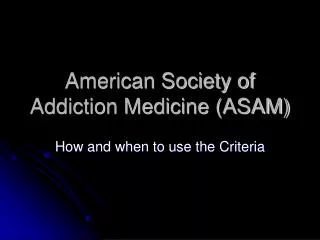
Case #2: “Lying to your doctor can be fatal” • Acutely precipitation of opioid withdrawal • DID NOT OCCUR, after an opioid antagonist was given in this case, • As it would have, if her initial HX was true. • And, by the way what did her MTD dosing curve look like??? • After all, she was only given 3 identical 20mg doses.
3 identical 20mg doses of MTD: - Given 24 hrs apart - To a pt who is NOT NEUROADAPTED (i.e. naïve) to the dose. Assume 100% absorption & average metabolism (i.e. pt is not a rapid nor slow metabolizer, & there are no drug interactions) 110 100 90 80 M T D 70 60 50 40 30 20 10 0 12 1 12 2 12 3 12 4 12 5 12 6 12 7 TIMEhrs/DAY
110 INTOXICATED AND ALMOST DEAD FROM VENTILATORY FAILURE 100 90 80 M T D 70 60 NALTREXONE 12.5mg given 50 40 30 NALTREXONE 25mg given 20 10 0 12 1 12 2 12 3 12 4 12 5 12 6 12 7 TIMEhrs/DAY
Acute Alcohol Withdrawal Syndrome (AWS) : • Signs & Symptoms : • Tachycardia • HT • Diaphoresis • Insomnia • Anxiety • N/V
Acute AWS : symptoms & signs • Tremor • Generalized SZ’s • Psychomotor agitation • Hallucinosis/delusions (+/- insight) • DT’s
AWS : Hallucinosis • Visual : • - lights too bright • - animal life: dogs, rodents, bugs in room
AWS : Hallucinosis • Auditory : • - sounds too loud/startling • - start out as unformed sounds • clicking • buzzing • thumping from other room • - may progress to formed voices
AWS : Hallucinosis • Auditory : • Formed voices • - friends/relatives • - accusatory in nature • In contrast to those of schizophrenia : • - religious • - political
AWS : Delusions • “I need to get dressed.” • “I need go to work.” • “I’ve got bills to pay.” • “I gotta get outa here.”
Acute AWS begins when Etoh levels start to fall, if the pt is neuroadapted to ETOH • Driven by : • Downregulation of inhibitory systems • Upregulation of excitatory systems • Dysregulating LC : NE output • Resultant hypernoradrenergic activity • From the brainstem.
AWS : withdrawal seizures (WD SZ’s) • Begin: 8 – 24 hrs AFTER LAST DRINK • May occur BEFORE a pt’s BAL=0 • Peak: 24 hrs after last drink • Type: grand mal (generalized) • singly, or in bursts • over a period of 1 – 6 hrs • Dilantin (phenytoin) is not effective Rx.
AWS : WD SZ’s • Risk of occurrence in pt’s with : • genetic predisposition • (+)Hx of prior WD SZ’s (“kindling”) • undergoing concurrent WD from : • - BZD’s • - BARB’s • - nonBARB sedatives (Soma / GHB)
DT’s • Generally appear 72 – 96 hrs • After last drink • That’s 3 – 4 DAYS AFTER LAST DRINK • lasting for an • ADDITIONAL 2 – 3 DAYS (rare > 50 d) • If someone starts into AWS + DT’s, • You’re looking at ONE WEEK.
CLASSIC DT’s • (+) all S&S’s of mild AWS, only now • SEVERE : • - tachycardia • - HT • - diaphoresis • - tremor • - fever
CLASSIC DT’s(cont.d) • - global confusion • - absorbed in a separate psychic reality • - believes him/her self to be in a location other than hospital • - may misidentify staff as personal acquaintances • - hallucinations without insight
CLASSIC DT’s(cont.d) • - marked psychomotor agitation • - efforts to get out of bed LASTING FOR HOURS • - absence of clear sleep LASTING FOR DAYS • Always monitor & Rx these pt’s • IN AN ICU
RISK OF DT’s : • (+) BAL > 300 mg/dl at presentation • (+) AWS seizure (SZ) at presentation
AWS Rx : • KEY : EARLY RX with BZD’s • To PREVENT potentially FATALDT’s • To shorten Rx time • Increase pt safety & comfort • Prevent intercurrent medical complications
BZD of choice : • Use : DIAZEPAM (Valium), PO/IV • NEVER : IM • - variable absorbtion with • - slow/undependable onset • - delayed respiratory depression • If IM BZD needed : LORAZEPAM (Ativan) • (Lorazepam may also be given IV)
Exception to Valium Rx : • Two groups of pts : • #1 = Elderly • #2 = Significant liver disease • - (GGT > 600) • - underlying active viral hepatits (HCV) • - hepatic cirrhosis
Exception to Valium Rx : • BOTH groups of pts have • reduced BZD elimination, but • CYP oxidative pathways • are reduced FAR MORE, than • the glucuronide conjugation pathways.
Exception to Valium Rx : • In these pts, use • Lorazepam (Ativan) • Oxazepam (Serax) • Because both drugs are • ALREADY 3-OH BZD’s • and therefore
Exception to Valium Rx : • only require glucuronidation • for elimination; and this avoids • ACCUMULATION of toxic/sedating • prodrug, or • intermediate active metabolites, • resulting from 2-keto BZD metabolism • (Valium/Librium are 2-keto BZD’s)
2-KETO BZD’s N-DESALKYLATED COMPOUNDS 3-OH BZD’s DEMOXEPAM (Long) TEMAZEPAM (RESTORIL) (Int) G L U C U R O N I D A T I O N CHLORDIAZEPOXIDE (LIBRIUM) (Intermediate) DIAZEPAM (VALIUM) (Long) NORDIAZEPAM (Long) OXAZEPAM (SERAX) (Int) TRIAZOLO BZD’s LORAZEPAM (ATIVAN) (Int) TRIAZOLAM (HALCION) (Short) ALPRAZOLAM (XANAX) (Short) ALPHA –OH’s via oxidation (Short) 7-NITRO BZD’s Nitroreduction & acetylation (NO ACTIVE METABOLITE) CLONAZEPAM (KLONOPIN) (Long)
REMEMBER : • All BZD’s reduce AWS symptoms, but • Diazepam, lorazepam, and clonazepam • Are better ANTICONVULSANTS • (because they have larger volumes of distribution, and are more lipophilic) • than either • chlordiazepoxide (Librium), or • oxazepam (Serax)
REMEMBER : • ALWAYS give Valium/Ativan • BEFORE the Haldol, • to eliminate/reduce risk of SZ’s from haloperidol
AWS Rx : Structured BZDDosing on med/surg floor • DIAZEPAM : • - 20mg PO q 6 hrs x 4 doses, then • - 10mg PO q 6 hrs x 4 doses, then • - 5mg PO q 6 hrs x 4 doses, then DC • Closely monitor pt • Give additional doses, or hold doses, • prn
AWS Rx : Structured BZDDosing on med/surg floor • LORAZEPAM : • - 2mg PO or IV q 6 hrs x 4 doses, then • - 1mg PO or IV q 6 hrs x 4 doses, then • - 0.5mg PO or IV q 6 hrs x 4 doses, then DC • Same precautions
AWS Rx : Symptom- Triggered BZD Protocol on a Chemical Dependency (CD) Unit • VALIUM : • 5-20 mg PO q 1-2 hrs, prn CIWA-r scale • Usually results in : • - 140mg Day #1 • - 70mg Day #2 • - 30mg Day #3 • None, or 5mg last day
AWS Rx : Symptom- Triggered BZD Protocol on a Chemical Dependency (CD) Unit
AWS Rx : Symptom- Triggered BZD Protocol • If agitation : • - Ativan 2-4mg PO/IM q 6 hrs • If psychotic symptoms : • - Ativan 2-4mg PO/IM q 6 hrs, then • - Haldol 2-5mg PO/IM q 6 hrs with • - Benadryl 50mg PO/IM q 6 hrs • If more than 1 dose Haldol given, then begin • - Cogentin 1mg PO q 12 hrs
AWS Rx : DT’s** • Ativan 1mg IV + Haldol 2mg IV, then • Ativan 2mg IV + Haldol 3mg IV, then • Ativan 3mg IV + Haldol 5mg IV • Q 20 MIN, going up scale, • IF NO RESPONSE to prior dose. • May repeat scale q 2-3 hrs, prn • Pt must be monitored in ICU
AWS Rx : DT’s • If not controlled with above, then • Paralyze • Completely sedate • Intubate & ventilate • Provide supportive ICU care • Hope pt does not die
Etoh Pharmacology :Elimination • Elimination Rate = 20 mg/dl, per hr, • in the serum, based on the BAL lab test. • The absolute amount of alcohol eliminated • from the body is 10 grams per hour, • or about the amount of alcohol in a “standard drink”
Etoh Pharmacology :Elimination • (BAL) + (20)(hrs since last drink) = Calculated BAL @ time of the last drink • Used to predict the SEVERITY of : • - impending AWS • - risk of DT’s, or SZ’s • during AWS.





![ADM-211 Exam Dumps - Preparation with ADM-211 Dumps PDF [2018]](https://cdn4.slideserve.com/7925318/salesforce-adm-211-exam-salesforce-certified-dt.jpg)