Download
1 / 94
950 likes | 1.03k Views
Understand the sudden onset of joint inflammation, its differential diagnosis, diagnostic studies like synovial fluid analysis, and management strategies for septic arthritis. Learn through a case study and essential information.

E N D
Clinical Approach to Acute Monoarthritis Mohammad Hasan Jokar
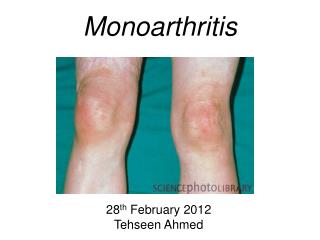
Acute Arthritis • The sudden onset of inflammation of the joint, causing severe pain, swelling, and redness. • Structural changes in the joint itself may result from persistence of this condition.
Signs of Inflammation • Swelling • Warmth • Erythema • Tenderness • Loss of function
Key Points • Distinguish arthritis from soft tissue non articular syndromes (discrepancy between “active” and “passive” ROM suggests periarticular/soft tissue) • If the problem is articular distinguish single joint from multiple joint involvement • Inflammatory or non-inflammatory disease • Always consider septic arthritis!
Acute Monoarthritis • Inflammation (swelling, tenderness, warmth) in one joint • Occasionally polyarticular diseases can present with monoarticular onset: (RA, JRA,Reactive and enteropathic arthritis, Sarcoid arthritis, Viral arthritis, Psoriatic arthritis)
Acute Monoarthritis - Etiology • THE MOST CRITICAL DIAGNOSIS TO CONSIDER: INFECTION ! • Septic • Crystal deposition (gout, pseudogout) • Traumatic (fracture, internal derangement) • Other (hemarthrosis, osteonecrosis, presentation of polyarticular disorders)
Questions to Ask – History Helps in DD • Pain come suddenly, minutes? – fracture. • 0ver several hours or 1-2 days? –infectious, crystals, inflammatory arthropathy. • History of IV drug abuse or a recent infection? – septic joint. • Previous similar attacks? – crystals or inflammatory arthritis. • Prolonged courses of steroids? – infection or osteonecrosis of the bone.
Indications for Arthrocentesis • The single most useful diagnostic study in initial evaluation of monoarthritis: SYNOVIAL FLUID ANALYSIS • 1. Suspicion of infection • 2. Suspicion of crystal-induced arthritis • 3. Suspicion of hemarthrosis • 4. Differentiating inflammatory from noninflammatory arthritis
Tests to Perform on Synovial Fluid • Total leukocyte count/differential: inflammatory vs. non-inflammatory. • Polarized microscopy to look for crystals. • Gram stain and cultures • Not necessary routinely: Chemistry (glucose, total protein, LDH) unlikely to yield helpful information beyond the previous tests.
Case 1 • 52 yo wm presents to the Emergency Department with a 2 day history of excrutiating pain, with swelling, of the left knee. He denies a history of trauma. He reports fever of 39 degrees and chills.
Physical Exam: T= 39.5 BP=150/92 P=105 RR=18The physical exam is notable only for the musculoskeletal exam which reveals:Left knee with erythema, warmth, and swelling. There is exquisite tenderness and pain with any motion. There is reduced range of motion due to pain. Other joints are normal.
The presentation of monoarticular arthritis *****Aspiration of the joint*****
Lab tests • CBC • Joint fluid study • Blood culture
Septic Arthritis • Key Features: • Monoarticular (almost always) • Dolor, rubor, calor • Swelling • Exquisite pain • Synovial fluid >50K WBCs and >95% PMNs • Aggressive disease warranting aggressive management
Septic Arthritis • Management of the patient with septic arthritis • Arthrocentesis • Hospital admission • Orthopedic consult • IV antibiotics • Broad spectrum antibiotics until culture and sensitivity available
Septic arthritis ******Drainage of the pus****** ******IV antibiotics are essential******
Septic Arthritis • Staphylococcus aureus - most aggressive • Rapid evolution to joint destruction • Importance of rapid diagnostic studies • Rapid initiation of therapy • Surgical drainage • Intravenous antibiotics
Epidemiology • 1:1 M:F • Mean Age=55 • 85%=Monoarticular • Patients with Damaged Joints are at Increased Risk • Most are hematogenously spread • Fever present in only 60% of non-GC septic arthritis • Crystalline arthritis is 4x as common as septic arthritis; fevers/rigors non-specific
Specific Infectious Agents • Causative agents identified in 2/3 of patients in whom suspected • 50% have known portal of entry • 25% are iatrogenic • 75% have extra-articular source: Look for skin, respiratory, or GU sources
Groups at risk for septic arthritis • Rheumatoid Arthritis: Account for up to 50% of cases • Immunosuppressed Host, especially Organ Transplant Patients • Advanced Age: Greater than 60, especially with Prosthetic Joints: May result in Osteomyelitis • Diabetes • Neoplasm • IV Drug Use: Repetitive transitory Bacteremia: Staphylococci (MRSA)>Enterobacter, Serratia, and Pseudomonas • Hemodialysis: Recurrent Vascular Infections, especially Staphylococci
Antibiotics and Supportive Therapy • Guided by local antibiotic sensitivity patterns • Intra-articular antibiotics are not required and may cause a chemical synovitis • Usually administered for 4 to 6 weeks • NSAID’s avoided until the diagnosis is secure • Joint Immobilization for 1 to 3 days • ROM as soon as possible
Case 2 • 22 yo wf presents to the Emergency Department with c/o left wrist pain of 2 days’ duration. She reports 2 weeks ago, the onset of left ankle pain and swelling which subsequently resolved in 3 days. She then developed 3 days of swelling and pain in the left knee, followed by 3 days of swelling and pain in the right knee.
Physical Exam • Temp 39 • Normal examination of HEENT, Lungs, CV, and Abdomen • Skin: Pustular lesions right 3rd and 4th fingers • Musculoskeletal: Left wrist warm, swollen (arthritis) with erythema extending along the extensor tendons of the hand (tenosynovitis)
Gonococcal Arthritis • Key Features • Migratory arthritis (immune mediated or reactive) • Tenosynovitis • Rash • Sexually active patient (though this may not be disclosed on history)
Gonococcal Arthritis • Evaluation • Aspiration of affected joint • Inflammatory joint fluid (>2000 WBC’s) • Rarely WBC count in the “septic” range (>50,000 WBC’s) • Cultures usually negative • Culture • Oropharynx, anus, cervix/urethra, skin lesions
Gonococcal Arthritis • Migratory Polyarthralgias/Polyarthritis/Tenosynovitis = 66%; Knee>hand>wrist • Dermatitis=sparse peripheral necrotic pustules in 40% • 83%=female, mean age=23, GU involvement in 63%, often asymptomatic • Check VDRL and HIV and Co-treat Chlamydia • DGI-like arthritis-dermatitis can also occur with H. influenzae, N. meningitidis, and S. moniliformis
Management • Antibiotics • Ceftriaxone • Doxycycline added (to cover likely concomittant Chlamydia infection) • Surgical drainage of the joint rarely necessary
Case3 • 32 y/o WM admitted to the hospital with 2 days of acute onset of arthritis in his right knee that progressed to the left knee. The day previous to the admission, he was evaluated in the ER, and an arthrocenthesis was attempted. The patient was discharged on ceohalexin 500 mg QID. • ROS: 3 weeks previous to admission he had an episode of diarrhea that lasted for 10 days and improved after treatment with Cipro. • Family History: Sister with recurrent uveitis.
Physical Examination • PE: fever 38.5. Otherwise within normal limits. • Joint exam: tenderness, redness and effusions in both knees. • Labs: ESR 60, Synovial fluid showed no crystals and Gram stain revealed no organisms. HLA B-27 positive. • Patient was started on indomethacin 50 mg PO QID with significant improvement of his symptoms.
Reactive Arthritis • “Reactive Arthritis (ReA) is an infectious induced systemic illness characterized by an aseptic inflammatory joint involvement occurring in a genetically predisposed patient with a bacterial infection localized in a distant organ/system”.
Reactive Arthritis • Epidemiology • ReA is an acute and insidious polyarthritis after an enteric and urogenital infections. • Incidence varies widely (1% to 20%). • Frequency varies from 0 to 15% after infection with Salmonella, Shigella, Campylobacter or Yersinia. • HLA-B27 can be present in 72% to 84% of the cases. • Incidence after Chlamydia trachomatis is not well known.
Reactive Arthritis • ReA can occurs in the absence of HLA-B27, this play a very important role.
Reactive Arthritis • Causative organisms • Frequent association: • Chlamydial trachomatis • Ureaplasma urealyticum • Salmonella enteritidis • Salmonella typhimurium • Shigella flexneri • Shigella dysenteriae • Campylobacter jejuni • Yersinia enterocolitica • Streptococcus SP
Reactive Arthritis • Less common association: • Chlamydia pneumoniae • Neisseria meningitidis serogroup B • Bacillus cereus • Pseudomonas • Clostridium difficile • Borrelia burgdorferi • Escherichia coli • Helicobacter pillory • Lactobacillus • Brucella abortus • Hafnia alvei
Reactive Arthritis • Clinical Manifestations: • Postenteric ReA is described equally in men an women. • Postchlamydial is most common in men. • In patients with postenteric ReA, the episode of diarrhea is usually prolonged. • Arthritis presents usually 2 to 3 weeks after the episode of diarrhea. • Arthritis usually resolves within 6 months, but a few patients had recurrences an a minority develops a chronic arthritis.