Download
1 / 39
420 likes | 754 Views
Image Gently, Step Lightly: Practice of ALARA in Pediatric Interventional Radiology. John M Racadio, MD 1 Bairbre Connolly, MB 2 1 Cincinnati Children’s Hospital Medical Center 2 The Hospital for Sick Children, Toronto. Why is this important?.

E N D
Image Gently, Step Lightly: Practice of ALARA inPediatric Interventional Radiology John M Racadio, MD1 Bairbre Connolly, MB2 1 Cincinnati Children’s Hospital Medical Center 2 The Hospital for Sick Children, Toronto
Why is this important? • In March, 2009, the National Council on Radiation Protection and Measurement released a critical report that indicated that radiation dose to the United States population had risen dramatically since the early 1980’s. • IR procedures are the third largest contributor to medical radiation to the US public. • Children are more sensitive to radiation effects and have a longer life span during which manifest possible changes as a result of radiation exposure. • Children who undergo interventional procedures may have a chronic illness and receive a higher lifetime cumulative dose secondary to repeat procedures and exposure. Kase KR (2009) Ionizing Radiation Exposure of the Population of the United States. National Council on Radiation Protection and Measurements, Bethesda, Maryland. Swoboda N, Armstrong D, Smith J, et al. (2005) Pediatric patient surface doses in neuroangiography. Pediatr Radiol 35:859-866. Rose S, Andre M, Roberts A, et al. (2001) Integral role of interventional radiology in the development of a pediatric liver transplantation program. Pediatr Transplant 5:331-338. Ahmed B, Shroff P, Connolly B, et al. (2008) Estimation of Cumulative Effective Doses From Diagnostic and Interventional Radiological Procedures in Pediatric Oncology Patients. Society for Pediatric Radiology, Scottsdale, Arizona. Thierry-Chef I, Simon S, Miller D (2006) Radiation dose and cancer risk among pediatric patients undergoing interventional neuroradiology procedures. Pediatr Radiol 36 Suppl 2:159-162.
ALARA • “As low as reasonably achievable” • General principle guiding radiation exposure • Keep radiation dose exposure to patient as low as reasonable for each procedure, given clinical need and patient factors
Learning objectives • Be familiar with practical strategies that are useful to reduce dose to patients & staff undergoing image guided procedures. • Learn about possible QA options to consider implementing in our own suites to improve our practice of radiation protection • Briefly describe some recent technologic advances and their impact on IR Dosimetry.
Practical Tips to Reduce Radiation Dose to Patients and IR Staff
Guiding Principles • Approach Radiation protection • patient and staff • Patient: Radiation dose is optimized when imaging is performed with the least amount of radiation required to provide adequate image quality and image guidance.
Guiding Principle • Staff: Scattered radiation in the room is directly proportional to the patient dose; if patient dose is reduced, so too is the dose to the operator and team. • To optimize radiation for the patient and minimize radiation for staff GOAL
Unique Features of Pediatric Intervention • Pediatric size (500gm – 100Kg) • Proximity of operator to the beam • Trade off: Need access to child but want hands out of the beam • Size of the I.I. relative to the child • Need for magnification ( dose) • Pediatric patient more radiation sensitive • Pediatric longevity • Use US where possible
In Practice How many times have we: • left our hands in the beam? • expediency over personal safety? • our backs to the X-ray source? • unaware of our foot on the pedal? • pushed away a protective barrier?
Proper Radiological Positioning* • Maximize distance between x-ray tube & patient. • Minimize distance between patient & Image Intensifier. • Stand on side of the Image Intensifier • Inverse square law – make use of it! * * Rad Techs play crucial role
Control Fluoroscopy • Collimate • Limit use to necessary evaluation of moving structures. • Employ last-image-hold to review findings • Unnecessary/Inadvertent fluoro – Make Aware! • Time bell warning • Reduce fluoroscopy pulses/sec to as low as possible/suitable (30/sec, 15/sec, 7.5/sec, 3.5/sec) • System in the room – increases dose awareness • IG Checklist ALARM PEMNET
Reduce Dose • Reduce field size (collimate) • Minimize field overlap. • Use low pulsed fluoroscopy • (7 or 3/sec) • Use low frame rate (4 or 2 or 1/sec) • Avoid unnecessary runs
Personal Protection - Hands • Keep hands out of the beam • Finger /ring badges • Angle of beam off hands • Collimation • Care
Control Images • Limit acquisition to what is essential for diagnostic and documentation purposes. • Last image hold • Think - Plan each run • Think - # frames / second • Think - magnification
Personal Protection - Shields • Lead table skirt / drape • Over head shields • Mobile Devices • Radioprotective non-lead patient drapes
I.I. I.I. Personal Protection – Awareness of Geometry • Maintain awareness of body position relative to the x-ray beam • Horizontal x-ray beam: operator and staff should stand on the side of the image receptor (I.I.) • Vertical x-ray beam: the image receptor should be above the table. • Angle beam where possible
Personal Protection - Wear • Well fitted lead apron (knees) • Leaded glasses (with sides) • Thyroid shield • Lead gloves – anesthetist - operator
Team Ergonomics* • Train operators and staff in ergonomics of the room - good positioning when using fluoroscopy equipment; periodically assess their practice. • Inverse Square Law • Front or Back lead • Identify and provide the best personal protective gear for operators and staff. • Acknowledge expertise & vigilance • of our technologists
Summary Goal To optimize radiation for the patient and minimize radiation for staff 1. AWARE 2. ALARA - Steps to reduce patient dose 3. ALERT - Steps to minimize staff dose
Potential Strategies to Optimize Radiation Exposure from Interventional Fluoroscopy
Ideal World • Clinical Success • The Least Amount of Radiation • Adequate Image Guidance • Established Practice Guidelines • Based on scientifically well designed studies.
Today’s Reality • Many IR procedures require high quality images, long fluoroscopy time or both. • There are NO consensus guidelines. • Practices vary from institution to institution, and even within an institution.
Where Can We Start? • Optimize operating parameters for x-ray machines. • Regularly inspect and maintain equipment. • Adequately train staff on equipment capabilities re: image quality and dose. • Develop QA and QC Dosimetry Programs
Equipment • Include Medical Physicist in decisions. • Machine Selection and Maintenance • Incorporate Dose-Reduction Technologies and Dose-Measurement Devices in equipment. • Establish Facility Quality Improvement Program • Appropriate x-ray equipment QA program • Overseen by a medical physicist • Equipment evaluation/inspection
Education and Training • Comprehensive Training of Operators • Radiation Biology, Physics, and Safety • Attend high-quality courses or complete a self-training course given by appropriate professional societies. • Comply with applicable state requirements.
Dosimetry Records • Measure and Record Patient Radiation Dose • Record Fluoroscopy Time • Record Available Measures • DAP (Dose Area Product) • Cumulative Dose • Skin Dose • Inform patients who have received high doses to examine x-ray beam entrance site for skin erythema.
Dosimetry Follow-UP • Develop Methods to Quantify Late Effects • Design medical records to clearly document the number and types of interventional procedures received by the patient. • Maintain a database of all patients with procedures and dose information. • Review dose information to identify patients with high doses (>3Gy) for follow-up. • Establish procedures for follow-up; including skin examination at 30 days.
Dosimetry Follow-UP CCHMC Policy: Machine – specific action level for patient call back based on 3 Gy (300 rad) entrance skin dose.
Physician-Patient Interactionpre-procedure • Ask patient about prior history of interventional fluoroscopy. • Communicate details of the procedure, patient dose, and immediate and long-term health effects to patients and their primary care providers. • Counsel patients on radiation-related risks, as appropriate, along with the other risks and benefits associated with the procedure.
Physician-Patient Interactionpost-procedure • Schedule a 30 day Follow-Up Visit if: • Radiation Skin Dose =/> 2 Gy, or • Cumulative Dose =/> 3 Gy • Send interventional fluoroscopy procedure description, operative notes, doses and information about the possible short-term and long term effects to the patient’s primary care provider. • The patient and primary care physician should be specifically requested to notify the operator if observable skin effects occur.
Monitor and ImproveOperator Performance • Audit outcomes of procedures (including patient radiation dose for each operator). • Share information learned in audits with operators and provide additional training as needed. • Provide annual radiation safety education for all operators. • Collaborate in clinical trials to identify best practices for optimizing doses to patients and minimizing dose to health care providers.
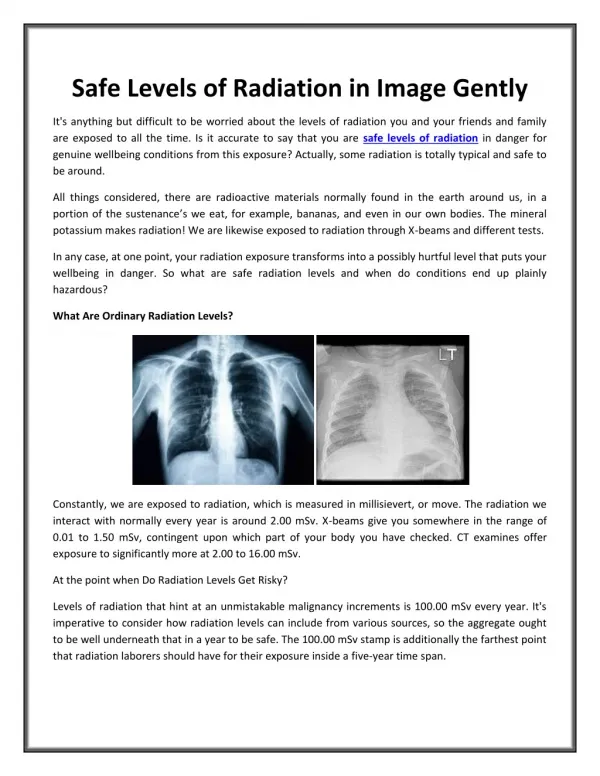
Technologic Advances • 3D Rotational Angiography • Flat Detector Systems • Cone Beam CT (“CT-Like Imaging”)
Cone Beam CT (“CT-Like Imaging”) These are NOT images from a CT. These are from IR flat detector c-arm
Our Collective Responsibility • More dosimetry studies in modern Pediatric IR suites need to be performed. • Manufacturers need to be made aware of the importance of limiting radiation exposure to children. • New technologies should be embraced, but dosimetry evaluation must be a priority.
References • Tsapaki V (2001) Patient and staff dosimetry problems in interventional radiology. Radiat Prot Dosimetry 94 :113-116. • Staniszewska MA, Jankowski J (2000) Personnel exposure during interventional radiologic procedures. Med Pr 51 :563-571. • Hidajat N, Vogl T, Biamino G, et al (1996) Radiation exposure in interventional radiology as exemplified by the chemoembolization of hepatocellular carcinoma and laser angioplasty of the pelvic arteries. Rofo 164 :249-256. • Meier N, Lenzen, H, Sudhoff A, et al (1995) Exposure of personnel in interventional radiology. Radiologe 35 :152-155. • NiklasonLT, Marx MV, Chan HP (1993) Interventional radiologists : ocupational radiation doses and risks. Radiology 187 :729-733. • Hall E (2002) Introduction to session I : Helical CT and cancer risk. Pediatr Radiol 32 :225.227. • Bacher K, Bogaert E, Lapere R, et al (2005) Patient-specific dose and radiation risk estimation in pediatric cardiac catheterization. Circulation 111 :83-89. • Swoboda NA, Armstrong DG, Smith J, et al (2005) Pediatric patient surface doses in neuroangiography. Pediatr Radiol 35 :859-866. • Streulens L, Vanhavere F, Bosmans H, et al (2005) Skin dose measurements on patients for diagnostic and interventional neuroradiology : a multicentre study. Radiat Prot Dosimetry 114 :143-146. • Fletcher DW, Miller DL, Balter S, Taylor MA (2002) Comparison of four techniques to estimate radiation dose to skin during angiographic and interventional radiology procedures. J Vasc Interv Radiol 13 :391-397. • Ropolo R, Rampado O, Isoardi P, et al (2001) Evaluation of patient doses in interventional radiology. Radiol Med 102 :384-390. • Vano E, Gonzalez L, Fernandez JM, Guibelalde E (1995) Patient dose values in interventional radiology. Br J Radiol 68 :1215-1220. • Miller DL, Balter S, Cole PE, et al (2003) Radiation doses in interventional radiology procedures; the RAD-IR study : part I : overall measures of dose. J Vasc Interv Radiol 14 :711-727. • van de Putte S, Verhaegen F, Taeymans Y, Thierens H (2000) Correlation of patient skin doses in cardiac interventional radiology with dose-area product. Br J Radiol 73 :504-513.
References • Faulkner K (2001) Dose displays and record keeping. Radiat Prot Dosimetry 94 :143-145. • King JN, Champlin AM, Kelsey CA, Tripp DA (2002) Using a sterile disposable protective surgical drape for reduction of radiation exposure to interventionalists. AJR Am J Roentgenol 178 :153-157. • Padovani R, Foti C, Malisan MR (2001) Staff dosimetry protocols in interventional radiology. Radiat Prot Dosimetry 94 :193-196. • Whitby M, Martin CJ (2005) A study of the distribution of dose across the hands of interventional radiologists and cardiologists. Br J Radiol 78 :219-229. • Jankowski J, Chruscielewski W, Olszewski J, Cygan M (2002) System for personal dosimetry in interventional radiology. Radiat Prot Dosimetry 101 :221-224. • Anderson NE, King SH, Miller KL (1999) Variations in dose to the extremities of vascular/interventional radiologists. Health Phys 76 :S39-40. • Vehmas T (1993) What factors influence radiologists’ finger doses during percutaneous drainages under fluoroscopic guidance? Health Phys 65 :161-163. • Pages J (2000) Effective dose and dose to the crystalline lens during angiographic procedures. JBR-BTR 83 :108-110. • Wyart P, Dumant D, Gourdier M, et al (1997) Contribution of self-surveillance of the personnel by electronic radiation dosemeters in invasive cardiology. Arch Mal Cœur Vaiss 90 :233-238. • Tsapaki V, Kottous S, Vano E, et al (2004) Occupational dose constraints in interventional cardiology procedures : the DIMOND approach. Phys Med biol 49 :997-1005. • Hayashi N, Sakai T, Kitagawa M, et al (1998) Radiation exposure to interventional radiologists during manual-injection digital subtraction angiography. Cardiovasc Intervent Radiol 21 :240-243. • National Cancer Institute and Society of Interventional Radiology (2005) Interventional fluoroscopy; reducing radiation risks for patients and staff. NIH publication no. 05-5286. • Cardella JF, Miller DL, Cole PE, et al (2003) Society of Interventional Radiology position statement on radiation safety. J Vasc Interv Radiol 14 :S387.