Download
1 / 23
230 likes | 246 Views
Learn about the .GUSTO-IV Pilot Trial focusing on improving reperfusion speed and outcomes in Acute Myocardial Infarction patients with novel combination therapies. The trial explores reducing mortality rates, enhancing safety, and facilitating early percutaneous interventions.

E N D
SPEED Rationale for Combination Therapy in AMI • Enhance Incidence and Speed of Reperfusion • Reduced Mortality • Safer Therapy - Less IC bleed • Facilitate Early Percutaneous Interventions ACC 1999: Oral Presentation
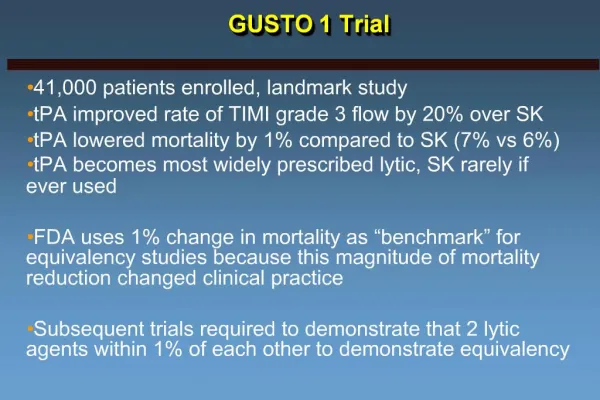
SPEED Rationale for Combination Therapy in AMI • Improved Reperfusion • Only 40-50% achieve normal perfusion (TIMI grade 3 flow) with fibrinolytic therapy alone • Reduced Mortality • 30% 1-year mortality among the elderly (> 75 years)in GUSTO-III ACC 1999: Oral Presentation
SPEED Rationale for Combination Therapy in AMI • Reduced ICH Rates • 21% increase in IC bleed from GUSTO-I to GUSTO-III with t-PA • Facilitate Early Percutaneous Interventions • Improved mortality with primary PCI is limited tohospitals where procedure and expertise is available ACC 1999: Oral Presentation
SPEED Overview of Trials of Low-Dose Lysis and GP IIb/IIIa Inhibitors TIMI -14 SPEED/GUSTO IV AMI Pilot Criteria Age 18 to 75 Symptoms < 12 hours > 18 years old Symptoms < 6 hours Control Arm(s) Accelerated t-PA and 10 U +10 U Reteplase Standard Reteplase 10 U +10 U Combination Therapies Studied t-PA, SK, or Reteplase + Reteplase + Abciximab* with Abciximab* with Heparin 60 U/kg 30 U/kg Heparin 60 U/kg 40 U/kg 1° Endpoint TIMI grade 3 flow at 90 minutes TIMI grade 3 flow at 60-90 minutes (avg. was 62 min) PCI “Encouraged” -Facilitated PCI Rescue only * bolus 0.25 mg/kg; infusion 0.125mg/kg/min x 12h ACC 1999: Oral Presentation
SPEED Ability of Abciximab to Cause Dethrombosis TIMI Grade 3 flow Study Time 25% 0 50% Gold et al 10 min Circ. 1997; 95: 1755-59 GRAPE 45 min JACC 1999; 33:1528-32 SPEED 60 min EHJ 1999; 20:616 (#3336) TIMI-14 90 min Circ. 1999; 99:2720-32 8% 18% 23% 32%
1:1 Randomization r-PA 10 + 10 U Heparin 70 U/kg Abciximab standard dose r-PA 5 + 5 U Heparin 60 U/kg / 40 U/kg 60-90 Minute Angiography PTCA + Stent as indicated SPEED Dose Confirmation Protocol • Acute MI • ST elevation • Symptom duration < 6 hrs. Administered in the ED ACC 1999: Oral Presentation
SPEED Dose Escalation and Confirmation Experimental Abciximab Abciximab + r-PA + r-PA 5 U + 5 U n = 166 60 U heparin n = 76 Control Abciximab Alone n = 63 Dose Escalation Experimental Abciximab Abciximab + r-PA 5 U + 5 U + r-PA 5 U + 5 U 60 U Heparin 40 U Heparin n = 40 n = 76 Control r-PA 10 U + 10 U n = 109 Dose Confirmation Total Abciximab + r-PA 5 U+ 5 U + 60U Heparin, n=116 ACC 1999; Oral Presentation
Dose ConfirmationAcute Cardiac Catheterization Abciximab r-PA 5 + 5 60 U Hep (n = 40) Abciximab r-PA 5 + 5 40 U Hep (n = 76) r-PA Alone (n = 109) Time from study 60 (50,65) 55 (48,61) 60 (48,67) drug to cath (min)* Infarct-related artery: LAD 41% 32% 45% LCX 14% 16% 9% RCA 44% 49% 45% PCI of IRA 83% 70% 94% at 60-90 min * median (25th, 75th) ACC 1999: Oral Presentation
SPEED TIMI Grade 3 Flow at 60-90 Min Angiographic Core Lab Reading by Treatment Recieved p = 0.395 n = 107 n = 34 n = 75 n = 109 r-PA Alone 60 U Hep Abciximab + r-PA 5 + 5 40 U Hep Abciximab + r-PA 5 + 5 Total ACC 1999: Oral Presentation
SPEED TIMI Grade 3 Flow at 60-90 Min Angiographic Core Lab Reading p = 0.06 p = 0.2 n = 107 n = 103 n = 75 n = 66 r-PA Alone 60 U Hep Abciximab + r-PA 5 + 5 40 U Hep Abciximab + r-PA 5 + 5 Abciximab Alone ACC 1999: Oral Presentation
SPEED Median TIMI Frame Count by Treatment Received Dose escalation and confirmation 100 p = 0.87 p = 0.43 43 36 33 60 U Hep Abciximab + r-PA 5 + 5 40 U Hep Abciximab + r-PA 5 + 5 Abciximab Alone r-PA Alone ACC 1999 : Oral Presentation
SPEED Clinical Outcomes* Abciximab r-PA 5 + 5 60 U Hep Abciximab r-PA 5 + 5 40 U Hep r-PA Alone Abciximab Alone Death 5.6% 4.4% 2.6% 3.2% Reinfarction 2.8% 1.7% 1.3% 0% Severe ischemia 2.8% 4.3% 2.6% 6.4% requiring urgent revascularization Composite 11.2% 9.6% 5.3% 9.5% * to 30 days post randomization ACC 1999: Oral Presentation
SPEED Rationale for Facilitated PCI • Meta-analyses suggest improved survival withprimary PTCA over lysis • Procedural success lower in vessels with TIMIGrade 0-1 vs. 2-3 • Limitations to primary PTCA include access(minority of hospitals can perform PCI) and delayin restoring flow (few hospitals < 60 min to cath) ACC 1999: Oral Presentation
SPEED Facilitated PCI 530 Patients 464 Patients 60-90 min cath TIMI Grade 0-1 (n = 136) TIMI Grade 2-3 (n = 324) 323 Patients PCI PCI 91% No PCI 9% PCI 61% No PCI 39% ACC 1999: Oral Presentation
SPEED Facilitated PCI Procedural Outcome Pre-Procedure TIMI Grade Flow 0-1 (n = 123) 2-3 (n = 198) Post-Procedure p Final diameter stenosis 10 (0, 25) 0 (0, 20) 0.0001 TIMI grade 3 flow 83% 95% 0.001 Stents 73% 81% 0.09 Procedural success* 81% 93% 0.001 * < 50% diameter stenosis with TIMI grade 3 flow ACC 1999: Oral Presentation
SPEED Facilitated PCI Clinical Outcome TIMI Grade Flow 0-1 (n = 123) 2-3 (n = 198) Death 4.1% 3.0% Reinfarction 2.4% 0.5% Severe ischemia 1.6% 1.5% requiring repeat revascularization Composite 7.3% 4.6% Blood transfusion 7.3% 10.1% ACC 1999: Oral Presentation
SPEED Facilitated PCI TIMI GRADE 2-3 Flow Early (60-90 min) PCI Late* PCI Abciximab alone 52% 83% 3% (n = 66) Abciximab + r-PA 5 + 5 76% 66% 11% (n = 192) r-PA alone 73% 61% 10% (n = 109) * > 24 hours after randomization ACC 1999: Oral Presentation
SPEED Facilitated PCI Procedural Outcome Abciximab Alone (n = 40) Abciximab + r-PA 5 + 5 (n = 114) r-PA Alone (n = 60) Post-Procedure p** Final diameter stenosis 10 (0, 25) 5 (0, 25) 5(0, 20) 0.41 TIMI grade 3 flow 95% 90% 85% 0.16 Stents 75% 75% 90% 0.02 Procedural success* 95% 88% 85% 0.35 * < 50% diameter stenosis with TIMI grade 3 flow ** compares any abciximab to r-PA alone ACC 1999: Oral Presentation
SPEED Facilitated PCI Clinical Outcomes Abciximab Alone (n = 40) Abciximab + r-PA 5 + 5 (n = 114) r-PA Alone (n = 60) Death 5.0% 5.3% 3.3% Reinfarction 0% 1.8% 1.7% Severe ischemia 5.0% 0.9% 1.7% requiring repeat revascularization Composite 10.0% 6.1% 6.7% Blood transfusion 5.0% 9.7% 6.7% ACC 1999: Oral Presentation
Conclusion • Low dose fibrinolytic therapy in addition to abciximab improves reperfusion rates • Heparin dose with the combination is also important to maximize reperfusion rates with abciximab + low-dose r-PA • Combination therapy appears to facilitateearly PCI in AMI
Results in a Perspective GUSTO-1 90-min Meta-analysis 60-min SPEED 60-min 100% p < 0.001 p = 0.06 14% 23% 23% 75% 54% 50% 31% 25% 0% Abciximab r-PA 5 + 5 SK t-PA ACC 1999: Oral Presentation
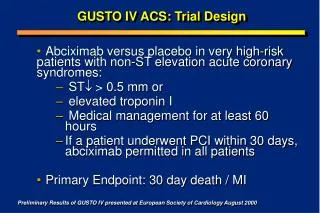
GUSTO-IV AMI Trial Protocol (n = 16,600) ST , lytic eligible, < 6 h ASA No Abciximab Abciximab* 2 x 10 U bolus (30’) Reteplase 2 x 5 U bolus (30’) Reteplase Standard Heparin: 5,000 U bolus followed by either 800 U/hr (pts < 80 kg) or 1,000 U/hr (pts > 80 kg) infusion Low Dose Heparin: 60 U/kg bolus followed by a 7 U/kg/h infusion 1º endpoint: mortality at 30 days 2º endpoint: clinical and safety events at 30 days * 0.25mg/kg bolus followed by 0.125 g/kg/min infusion for 12 hours