Download
1 / 28
330 likes | 822 Views
Risk Stratification in CVD Prevention How to Identify Cardiovascular Risk in the Office. Dr. Thomas G. Allison Cardiovascular Diseases and Internal Medicine Mayo Clinic Rochester, MN. Clinically-Based CVD Prevention. Risk assessment for all patients

E N D
Risk Stratification in CVD PreventionHow to Identify Cardiovascular Risk in the Office Dr. Thomas G. Allison Cardiovascular Diseases and Internal Medicine Mayo Clinic Rochester, MN
Clinically-Based CVD Prevention • Risk assessment for all patients • Set evidence- and guideline-based goals for specific risk factors • Lifestyle management • Pharmacologic intervention for selected risk factors in appropriate patients
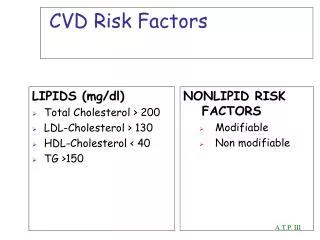
Levels of Risk in Primary Prevention • Highest: the patient has evidence of CVD • High: the patient has high immediate risk (a probability of > 20% in the next 10 years) for having a CVD event • 2 or more major risk factors BP > 160/100 Diabetes Cigarette smoking LDL cholesterol > 160 mg/dL HDL cholesterol < 35 mg/dL men, < 45 mg/dL women Family history of premature CVD
Levels of Risk in Primary Prevention • Intermediate: the patient will not likely have a CVD event in the next 10 years, but has a high lifetime risk • 1 major risk factor or • > 2 minor risk factors BP 140-159/90-99 mmHg Blood glucose 100-129 mg/dL LDL cholesterol 130-159 mg/dL HDL cholesterol 35-39 mg/dL men, 45-49 mg/dL women
Levels of Risk in Primary Prevention • Low: the patient may develop CVD at older ages without lifestyle adjustment • 1 or 2 minor risk factors • Minor risk factors are generally correctable with lifestyle change • Diet change, exercise, weight loss • Very low: the patient will not likely develop CVD during his or her lifetime • No major or minor risk factors
What Do We Do with Risk? • Highest risk patient • Use secondary prevention guidelines to manage risk factors • Further evaluation: exercise test ± imaging or angiography • High risk patient • Treat all major risk factors pharmacologically • Provide appropriate lifestyle counseling • Exercise test
What Do We Do with Risk? • Intermediate risk patient • Lifestyle counseling • Pharmacologic treatment of any major risk factors • Initial follow-up in 3-6 months, annually thereafter • Consider exercise test
Stress Testing for Risk Stratification in Primary Prevention • Look for clinical disease • Evaluate symptoms • Establish prognosis • Prior to prescribing exercise • Intermediate-high risk patients • High threshold of disease
What Do We Do with Risk? • Low risk patient • Recommend appropriate lifestyle change • Re-evaluate in 3-12 months • Very low risk patient • Reassure • Suggest additional evaluation in 3-5 years
Prediction of Lifetime Risk for Cardiovascular Disease by Risk Factor Burden at 50 Years of Age Donald M. Lloyd-Jones et al Circulation 2006;113:791-798
High Intermediate Low Very Low
Identifying Risk in the OfficeStep 1 • Symptoms: Angina, TIA, claudication • Physical exam: bruits, AAA, diminished peripheral pulses, reduced ABI (0.90 for men and 0.85 for women), xanthomas • ECG: Q-waves, ST-T wave abnormalities, LVH
Angina has 3 characteristics • Feels like tightness, pressure, squeezing, or burning (not generally a sharp pain) • Starts in the center of the chest, behind or underneath the sternum (breast bone) – may radiate to the neck and jaw, around the back, down the arms (left more common than right) • Increased by physical activity, relieved by rest (or nitroglycerine)
Rose Angina Questionnaire • 1. Do you get pain or discomfort in your chest when walking up hills, stairs or hurrying on level ground? (Yes or no) Positive = “yes” • 2. If you get pain or discomfort in the chest when walking, do you usually stop? Slow down? Carry on at the same pace? (Mark the alternative best fitting) Positive = “stop” or “slow down” • 3. If you stop or slow down, does the pain disappear after less than 10 minutes? Or after 10 minutes or more? (Mark the alternative best fitting) Positive = “after less than 10 minutes”
Other symptoms that might represent coronary heart disease include • Fatigue • Reduced exercise tolerance • Shortness of breath • Symptoms suggesting other vascular disease • TIA • Claudication
Assessing CVD Risk in the OfficeStep 2 • Measure height, weight, waist circumference, calculate BMI • Measure blood pressure and pulse • Discuss family history of premature CVD • Review lifestyle: smoking, physical activity, diet (servings of fruits/vegetables per day)
Non-Fasting Blood Sugar, Lipids • Physicians in developing countries (or in low income populations in developed countries) may not have the luxury of scheduled visits for measurement of fasting blood sugar and lipids • Inexpensive, fingertip, glucometer • Opportunities for measuring these factors in non-fasting states will present
Non-Fasting Blood Sugar • In routine cases where patient is not fasting but not acutely ill, FBG > 150 mg/dL may serve to identify patients with diabetes or impaired fasting glucose • Consider measuring hemoglobin A1C • Reflects status prior to acute illness • May underestimate prevalence of diabetes • Elevated A1c indicates need to begin therapy
When to Add a Lipid ProfileStep 3 • Positive family history of CVD • BMI > 28 kg/m2 or prominent waist circumference (> 102 cm men, 89 cm women) • High non-fasting glucose • Improper dietary habits • Elevated blood pressure • Cigarette smoking • Consider for all patients if resources available
Honduras versus US Statistics • Total expenditure on health per capita • Honduras: $241 US: $6,714 • Gross national income per capita • Honduras: $3,240 US: $44,070 • Total expenditure on health as % of GDP • Honduras: 7.4% US: 15.3% World Health Statistics 2008 Financial data from 2006
Fasting Lipid Profile?Non-HDL Cholesterol • Easy to calculate: Total-C – HDL-C • Predicts CVD risk as well as LDL-C • Goals = LDL-C goals + 30 mg/dL • Not much affected by non-fasting samples • Can be used opportunistically
More Tools for Assessing CHD Risk in Asymptomatic Adults • Novel risk factors (CRP, Lp(a), Lp-PLA2, etc.) • Advanced lipid testing • LDL particle concentrations, apolipoproteins • Non-invasive imaging • EBCT, CIMT, CTA, MRI • Arterial function studies • Brachial reactivity, ENDO-PAT, arterial stiffness
Framingham Risk Score • Very age dependent • Short-term (10-year) risk projections • Ignores many factors that likely contribute to cardiovascular risk • Developed in USA with people of (western) European descent • Does it have to be modified for developing nations or different racial or ethnic groups?
Framingham 10-year risk by age for a male or female ●smokes 1 ppd ●TC = 212 (5.5), HDL-C = 42 (1.1) ●No DM, normal BP
Three Options for Preventing CVD in Asymptomatic Individuals • Wait until the patient has had a CVD event • Wait until the patient has signs of atherosclerosis • Requires expensive imaging procedures • Treat factors that lead to an increased lifetime risk of CV disease • How do we know when it is time to start? • Likely 10-20 years earlier than current practice
Comments? • Questions?