Download

1 / 28
290 likes | 426 Views
Michiel Bähler. FACT Teams in the heart of the organization for persons with a SMI. Welcome to the Netherlands 16 M inhabitants /. FACT NHN . 3. Rural. Urban problems. 1997 . Start deinstitutionalization ICM model, outreaching 2002 / 2003, Evaluation

E N D
Michiel Bähler FACT Teams in the heart of the organizationfor persons with a SMI
Welcome to the Netherlands16 M inhabitants / FACT NHN 3
1997 • Start deinstitutionalization • ICM model, outreaching • 2002 / 2003, Evaluation • Care was outreaching, supportive • Almost no CPN, no doctors, • Crisisintervention to late • Long admission, no contact CM during admission
Cinderella and SMI • Care is fragmented • Evidence not available • Not much connection in organisation • No evaluation
Cure and Care for SMI Long stay Social security Spec outpatient clinic Acute ward Day hospital sheltered housing Alcohol & Drugs CM Public MH team General Hospital Rehab Crisis NGO day act centre
2003 • Introduction ACT in Netherlands • NHN • 2 ACT teams / 10 CM teams • Dilemma • ACT leaves out 80% of the SMI. • Graduation to step down teams, discontinuity • Returning in ACT FACT NHN
FACT Long stay Acute ward Sheltered housing Alcohol & Drugs Public MH General Hospital Crisis Dagactivity-centre FACT teams
FACT: a Dutch version of ACT • Instead of ACT and CM teams FACT • increasing continuity of care • flexible response (2 levels of intensity) • regional teams » social inclusion • ‘transmural’: linking hospital & community care
Innovation • Flexible ACT (FACT) offers care and treatment to 100% of SMI-population in a catchment area: • FACT teams are working with TWO procedures; • Lower scale: state of the art treatment (offered by intensive casemanagement from a multidisciplinary team) • High scale: Full ACT with shared caseload by the same multidisciplinary team • Procedure for up- and downgrading of care
FACT in GGZ-NHN • 600.000 inhabitants • 12 FACT teams • Substance abuse clinic • Acute wards • Sheltered living
‘ACT – Teams’ in NL • ACT (mainly in large cities) • Flexible ACT • Early Intervention Psychosis • Forensic (F) ACT FACT NHN
Six principles FACT
Ad1) FACT-board • Digital FACT BOARD • Shared Caseload • Shared knowledge / ideas FACT NHN
Indications for ‘admission to’ the FACT board • Temporary • Long term & Revolving door • Difficult to engage • Admission (Psychiatry / Gen. Hosp / Jail) • Legal (outpatient commitment) FACT NHN
Ad 2): EBP treatmentservice delivery model • Medication + Medication Management • Metabolic Syndrome • Cognitive Behaviour Therapy • Family intervention • Psycho-education • Supported Employment ( IPS) • IDDT FACT NHN
Ad 3) Recovery • Promoting: • Person-centered • Strengths- based • Collaborative • Empowering • Respect and Hope FACT NHN
Ad4) Binding the MH • Continuity of care between community and hospital • FACT team is responsible for treatment plan, also during admission • During admission, Care coordination meeting (CCM) client, family, CM FACT-team and team ward about goals of admission and length of stay
Ad 5) FACT and the community • The region-focussed model provides good conditions for community care • Being in close contact with neighbourhood, G.P. and police • Accessible / Case-finding • Working with (individual) support systems on inclusion • Use naturally occurring resources
Ad 6) • We will be there were the clients wants to be succesfull • “Place than train principle” • E.g. supported employment
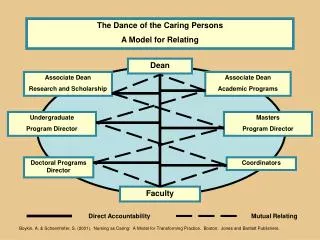
Rich Multidisciplinary team • Team (+/- 11 FTE) for 160 – 180 patients: • (community) psychiatric nurses • 0.8 – 1.0 psychiatrist • Psychologist • Peer specialist, • Social worker, • Substance Abuse (IDDT) • Supported employment specialist (IPS) • Manager / team leader