Download
1 / 12
140 likes | 640 Views
HODGKIN LYMPHOMA . Classifications. 1%. Hodgkin lymphoma. 1% of all cancers Arises in lymph nodes (tons., Wald., EXN rare) Spreads predictably characteristically to the anatomically contiguous nodes LN – spleen – liver – BM Staging: prognosis, choice of therapy. Patients.

E N D
Classifications • 1%
Hodgkin lymphoma • 1% of all cancers • Arises in lymph nodes • (tons., Wald., EXN rare) • Spreads predictably • characteristically to the anatomically contiguous nodes • LN – spleen – liver – BM • Staging: prognosis, choice of therapy
Patients • Average: 32 years; slight male predominance • (NS: M=F) • Curable in many cases • Lon-term survivors of chemo- and radiotherapy: • Risk of developing second cancers • MDS, AML, lung cancer, breast cancer
HODGKIN LYMPHOMA WHO 2008 • CLASSICAL (95%) • NODULAR LYMPHOCYTE PREDOMINANT (nodular paragranuloma, 5%) DIFFER IN: TUMOUR CELLS BACKGROUND CLINICAL FEATURES
CLASSICAL HL SUBTYPES NODULAR SCLEROSIS MIXED CELLULARITY LYMPHOCYTE RICH LYMPHOCYTE DEPLETION FEATURES • COMMON TUMOUR CELLS • DIFFERENT BACKGROUND ARCHITECTURE CLINICAL, EPIDEMIOLOGY EBV
TUMOUR CELLS OF CLASSICAL HL Diagnostic only RS! Hodgkin cell CD30+,CD15+ B-markers, EBV mummy lacunar eggs in the basket
Classical HL NODULARSCLEROSIS 70% CHL; 28 ys; M=F stage II, mediastinum 40% B-symptoms grade I and II MIXED CELLULARITY 20% CHL; 37 ys; 70% M stage III-IV peripheral lymph nodes spleen, bone marrow B-sympt., EBV common HIV
Classical HL LYMPHOCYTE RICH 5% CHL; older; 70% M stage I-II peripheral lymph nodes B-sympt. rare, but relapses LYMPHOCYTE DEPLETION <5% CHL; 37ys; 75% M advanced B-symptoms common poor, HIV (EBV)
Nodular lymphocyte predominance HL CD20 Nodular/diffuse pattern L&H; LP = popcorn cells Background FDC meshworks nonneoplastic lymphocytes Very favourable prognosis
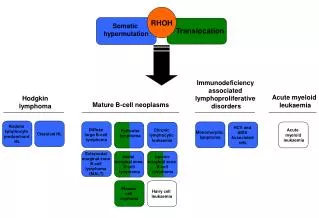
Reed-Sternberg cell: communication with other cell types
I, II above diaphragm below III, IV Hodgkin lymphoma – Ann Arbor staging Pruritus, anorexia; B sympt. correlate with stage