Download
1 / 23
550 likes | 2.88k Views
What is scapular dyskinesis?. Scapular dyskinesis is the alteration of the normal static or dynamic position and the motion of the scapula during scapulohumeral movements. Scapular dyskinesia alters the scapulohumeral rhythm due to weak scapular and rotator cuff musculature.This can cause shoulder

E N D
1. Scapular Dyskinesis Rehabilitation By Kristen Knorr
2. What is scapular dyskinesis? Scapular dyskinesis is the alteration of the normal static or dynamic position and the motion of the scapula during scapulohumeral movements.
Scapular dyskinesia alters the scapulohumeral rhythm due to weak scapular and rotator cuff musculature.
This can cause shoulder pain in a number of ways due to the malfunctioning of the scapula.
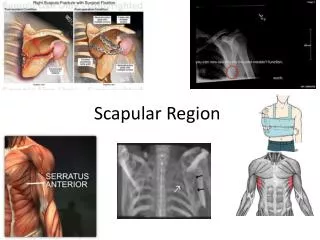
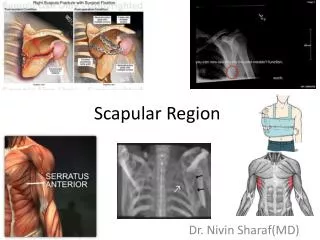
3. Shoulder Girdle Anatomy:
4. Shoulder Girdle Anatomy:
5. Scapular Stabilizers: Trapezius
Serratus Anterior
Rhomboids
Levator Scapulae
Latissimus dorsi
6. Scapular dyskinesis: There are 4 types:
Type 1 � inferior angle prominence
Type 2 � medial border prominence
Type 3 � superior angle elevation
Type 4 � symmetric pattern
7. The �SICK� Scapula: The term SICK scapula is another way to describe scapular dyskinesis.
SICK scapula - the pathological state of the scapula characterized by scapula mal position, inferior border prominence, coracoid pain and mal position and kinesis abnormalities of the scapula.
8. Common Sports: Scapular dyskinesis is most common in baseball pitchers and swimmers. Although all overhead athletes are prone to this dysfunction.
9. Associated Injuries: Dysfunction in scapular position and mechanics is seen in:
100% of cases of glenohumeral instability
68% of those with abnormalities to the rotator cuff
94% with labral tears.
10. Rehabilitation: Early rehabilitation should aim to improve the endurance and strength of the scapular stabilizers.
Low weight, high repetition exercises promote muscle hypertrophy and improve fatigue resistance.
Once more normal scapular mechanics have been restored, higher weights with lower repetitions may be used to promote power.
Rotator cuff strengthening can begin once a stable scapular base has been restored
11. Rehabilitation: Once endurance and strength have improved, exercises that promote effective energy transfer through the kinetic chain should be added
Proprioceptive Neuromuscular Facilitation helps promote normal scapulohumeral rhythm and improve the body�s ability to position the scapula for stable energy transfer during functional activities.
12. Phase 1: Muscle Strengthening and Conditioning Avoid any motions that cause pain and use ice to control pain and inflammation
ROM: 3 x 30 secs.
Cross Body Adduction
Sleeper Stretch
Manual Internal Rotation
Pectoralis Major
13. Phase 1: Scapular Stabilizer Strengthening with rubber tubing, manually, dumbbells or machines.
Isometric scapular retraction
Shoulder shrugs
Seated rows w/ retraction
Prone rows
Push ups w/ a plus
14. Phase 1: Bench press w/ a plus
Seated flys
Lat pull downs
Elevation
Protraction
Depression
Retraction
15. Phase 2: Continue anterior stretching
Add biceps and IR stretching
Continue all scapular exercises while increasing weight, reps, etc
Can begin an upper body ergometer
Cybex if available
16. Phase 2: Rotator Cuff Strength w/ dumbbells or tubing. 3 x 10.
internal and external rotation at 0 and 90
Abduction to 90
Scaption (empty can)
Chest pass w/ a medicine ball
PNF patterns ( D1, D2 flexion and extension)
Rhythmic Stabilization (closed chain)
17. Phase 2: Phillie�s shoulder series
Thumb tacks
Train whistles
Statue of liberty
18. Phase 3: The upper body ergometer should increase resistance and can be done both forward and backward
Weights and resistance should be increasing for all exercises.
Prone rows can be done on a swiss ball
Rhythmic stabilization can be done with eyes open, eyes closed and supine
19. Phase 3: Sport specific work should begin
Throwing technique should be corrected and should start with short distance throws.
For other sports they should be able to block, tackle, pass, shoot, etc with no pain.
20. Functional Activity: All components of the patients sport should be pain free and with correct techniques.
This can be tested by doing each skill of the sport and comparing their motion.
The patient should no longer have any abnormalities when observing the scapula ( no inferior angle, medial border, or superior angle prominence)
21. Functional Activity: Cybex: if available this can be used to determine the strength of the shoulder and whether they are strong enough to return to play.
22. Summary: Scapular dyskinesis is a malfunctioning of scapular movement that can affect the entire shoulder.
It is most commonly seen in baseball pitchers and swimmers.
Strengthening should be focused on scapular stabilization as well as rotator cuff musculature.
23. Questions?