Download
1 / 1
10 likes | 90 Views
Explore the impact of self-reported disability on trunk muscle activity during isometric trunk exertions in chronic low back pain patients. Study compares muscle activations in different movement patterns.

E N D
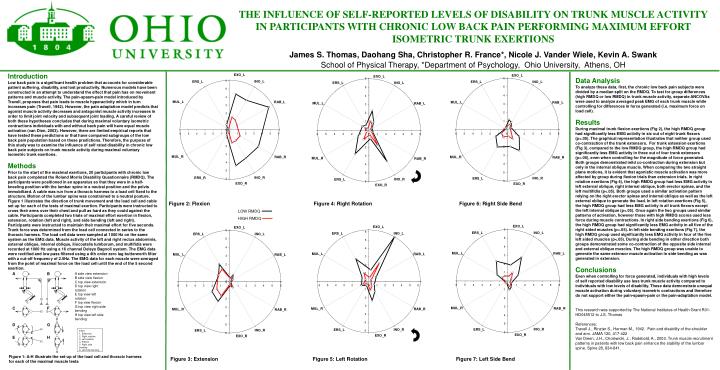
A B A side view extension B side view flexion C top view extension D top view right rotation E top view left rotation F top view flexion G top view right side bending H top view left side bending C F D G Effort 1. Extension 2. Right rotation 3. Left rotation 4. Flexion 5. Right side bending 6. Left side bending E H THE INFLUENCE OF SELF-REPORTED LEVELS OF DISABILITY ON TRUNK MUSCLE ACTIVITY IN PARTICIPANTS WITH CHRONIC LOW BACK PAIN PERFORMING MAXIMUM EFFORT ISOMETRIC TRUNK EXERTIONS James S. Thomas, Daohang Sha, Christopher R. France*, Nicole J. Vander Wiele, Kevin A. Swank School of Physical Therapy, *Department of Psychology, Ohio University, Athens, OH Introduction Low back pain is a significant health problem that accounts for considerable patient suffering, disability, and lost productivity.Numerous models have been constructed in an attempt to understand the effect that pain has on movement patterns and muscle activity. The pain-spasm-pain model introduced by Travell, proposes that pain leads to muscle hyperactivity which in turn increases pain (Travell, 1942). However, the pain adaptation model predicts that agonist muscle activity decreases and antagonist muscle activity increases in order to limit joint velocity and subsequent joint loading. A careful review of both these hypotheses concludes that during maximal voluntary isometric contractions individuals with and without back pain will have equal muscle activation (van Dien, 2003). However, there are limited empirical reports that have tested these predictions or that have compared subgroups of the low back pain population based on these predictions. Therefore, the purpose of this study was to examine the influence of self rated disability in chronic low back pain subjects on trunk muscle activity during maximal voluntary isometric trunk exertions. Methods Prior to the start of the maximal exertions, 20 participants with chronic low back pain completed the Roland Morris Disability Questionnaire (RMDQ). The participants were positioned in an apparatus so that they were in a half-kneeling position with the lumbar spine in a neutral position and the pelvis immobilized. A cable was run from a thoracic harness to a load cell fixed to the structure. Motion of the lumbar spine was constrained to a neutral posture. Figure 1 illustrates the direction of trunk movement and the load cell and cable set up for each of the tests of maximal exertion. Participants were instructed to cross their arms over their chest and pull as hard as they could against the cable. Participants completed two trials of maximal effort exertion in flexion, extension, rotation (left and right), and side bending (left and right). Participants were instructed to maintain their maximal effort for five seconds. Trunk force was determined from the load cell connected in series to the thoracic harness. The load cell data were sampled at 1000 Hz on the same system as the EMG data. Muscle activity of the left and right rectus abdominis, external oblique, internal oblique, iliocostalis lumborum, and multifidis were recorded at 1000 Hz using a 16 channel Delsys Bagnoli system. The EMG data were rectified and low pass filtered using a 4th order zero lag butterworth filter with a cut-off frequency of 2.5Hz. The EMG data for each muscle were averaged from the point of maximal force on the load cell until the end of the 5 second exertion. Data Analysis To analyze these data, first, the chronic low back pain subjects were divided by a median split on the RMDQ. To test for group differences (high RMDQ or low RMDQ) in trunk muscle activity, separate ANCOVAs were used to analyze averaged peak EMG of each trunk muscle while controlling for differences in force generated (i.e. maximum force on load cell).Results During maximal trunk flexion exertions (Fig 2), the high RMDQ group had significantly less EMG activity in six out of eight trunk flexors (p<.05). The graphical representation illustrates that neither group used co-contraction of the trunk extensors. For trunk extension exertions (Fig 3), compared to the low RMDQ group, the high RMDQ group had significantly less EMG activity in three out of four trunk extensors (p<.05), even when controlling for the magnitude of force generated. Both groups demonstrated mild co-contraction during extension but only in the internal oblique muscle. When comparing the two straight plane motions, it is evident that agonistic muscle activation was more affected by group during flexion trials than extension trials. In right rotation exertions (Fig 4), the high RMDQ group had less EMG activity in left external oblique, right internal oblique, both erector spinae, and the left multifidis (p<.05). Both groups used a similar activation pattern relying on the right erector spinae and internal oblique as well as the left external oblique to generate the load. In left rotation exertions (Fig 5), the high RMDQ group had less EMG activity in all trunk flexors except the left internal oblique (p<.05). Once again the two groups used similar patterns of activation, however those with high RMDQ scores used less force during muscle contractions. In right side bending exertions (Fig 6), the high RMDQ group had significantly less EMG activity in all five of the right sided muscles (p<.05). In left side bending exertions (Fig 7), the high RMDQ group used significantly less EMG activity in four of the five left sided muscles (p<.05). During side bending in either direction both groups demonstrated some co-contraction of the opposite side internal and external oblique muscles. The high RMDQ group was unable to generate the same extensor muscle activation in side bending as was generated in extension. Conclusions Even when controlling for force generated, individuals with high levels of self reported disability use less trunk muscle activity compared to individuals with low levels of disability. These data demonstrate unequal muscle activation during voluntary isometric contractions and therefore do not support either the pain-spasm-pain or the pain-adaptation model. This research was supported by The National Institutes of Health Grant R01-HD045512 to J.S. Thomas References: Travell J., Rinzter S., Herman M., 1942. Pain and disability of the shoulder and arm. JAMA 120, 417-422 Van Dieen, J.H., Cholewicki, J., Radebold, A., 2003. Trunk muscle recruitment patterns in patients with low back pain enhance the stability of the lumbar spine. Spine 28, 834-841. Figure 2: Flexion Figure 4: Right Rotation Figure 6: Right Side Bend LOW RMDQ HIGH RMDQ Figure 3: Extension Figure 1: A-H illustrate the set-up of the load cell and thoracic harness for each of the maximal muscle tests Figure 5: Left Rotation Figure 7: Left Side Bend






