Download
1 / 24
240 likes | 308 Views
Physician Oversight of EMS and Interface with Quality Processes. Roger M. Stone, M.D.,M.S., FAAEM, FACEP Faculty, Department of Emergency Medicine University of Maryland School of Medicine Medical Director, Montgomery Co Fire & Rescue

E N D
Physician Oversight of EMS and Interface with Quality Processes Roger M. Stone, M.D.,M.S., FAAEM, FACEP Faculty, Department of Emergency Medicine University of Maryland School of Medicine Medical Director, Montgomery Co Fire & Rescue Associate Medical Director, Carroll County Emergency Services Association UMBC / UMB EMS Fellowship
Objectives • Definitions and terminology relating to physicians in EMS • History • Stages of input: Prospective, Immediate, Retrospective • Understand focus on medical quality process • Quality as primary mission of Medical Director • Describe roles in on-line medical oversight • Describe potential role in peer review • Typical types of calls requiring direction
Brief History • Important: Genesis of BLS • The Institute of Medicine’s “White Paper” • Accidental Death and Disability: The Neglected Disease of Modern Society (1966) • BLS previous to the White Paper • Hearses or loose tiered ambulances, scoop & run • Variable training in First Aid, little physician input • After the EMS Act of 1973 • Monies available to create systems, including training • Formal BLS was born from this
History of ALS • Genesis: CPR in Baltimore • Dr. Peter Safar (JHU 1950s) • St Vincent’s Mobile CCU in NYC • Dr. William Grace and CCU Fellows~ 1969 • Seattle Medic One • Dr. Leonard Cobb (U Washington 1970) • Miami Fire Department Rescue One • Dr. Eugene Nagel (U Miami 1969)
History of Physicians in EMS • Medical Command/Control (50’s-70’s) • Medical Direction in late 80’s to early 90’s • EMS got more autonomous • “EMS Physician” was born (circa 1986-90) • origin: Nat’l Assoc EMS Physicians (NAEMSP) • Position Paper on Medical Oversight (1998) • Medical Oversight • most modern terminology • Source: Prehospital Care and Medical Oversight (NAEMSP)
Definitions of Medical Oversight • The responsibility of physicians to direct the prehospital system and providers in the overall clinical management of patients E. Racht • The result of the legal, moral and medical authority responsible for the provision of pre-hospital care by physician extenders • A process whereby a physician director insures that care provided to patients by the EMS system is both appropriate and beneficial - R. Bass • The implementation & supervision by a physician of the medical aspects of a system designed to deliver emergency patient care in the out of hospital setting • R. Stone
Stages of Medical Input • Stages of Input • Retrospective • Immediate • Prospective
Retrospective Input • Results from the review of individual calls and collected data • to determine if the system is working…not! • Assesses that appropriate skills were used and maintained (ex IVs, ETT) • Proactive problem solving & QI possible • Peer review if individual personnel err
Prospective Input • Involvement prior to actual events • training of providers • patient care guidelines/standards/protocols • equipment selection and approval • appropriate credentialing of providers • Quality measures in place in advance
Immediate Input • Also referred to as On-Line Oversight • Only 2 major mechanisms • Radio Communication • On scene physician (3 types) • System EMS physician • Patient’s physician • Stranger/Samaritan/Passer-by
Levels of Care • 1st Responder • Emergency medical Technician-Basic • Emergency Medical Technician- Intermediate (300+ hours) • Emergency Medical technician-Paramedic (600-900 hours)
What should Residents know about EMS quality systems? • Need existence of state law enabling EMS • Regulations: Guide Local and State QI • Ability to query data in order to improve • Inquiry process & peer review mechanism • MD subtitles guide all aspects of EMS • 02:Providers;03:Programs;04:Education • 05: Regions; 06:AED; 07:Syscom; 08:Centers • Source Maryland COMAR Title 30
Base Stations • Cornerstone of on-line direction • Source COMAR Title 30, Subtitle 03, Chapter 06 • Surrogate for the medical director’s inability to be everywhere all the time • Residency trained front line EPs, 24h/7d • Has a mandate for quality consultations
What should EM residents know about the medical director? • The medical director is hybrid: • Independent voice of off-line direction • Not an agent of either management or rank and file • Not agent of State, but subject to laws or regulations • Works with leaders, but nurtures rank & file • Looked upon as a mentor on the medicine • Future EM graduates may be asked: • “Doc, could you be our medical director?”
Task Areas: Scope of Medical Practice ! Authority to impact quality of care • Medical decisions about assessment & treatment protocols, as well as equipment • Medical support for dispatch protocols • Medical consultant for training programs • Authority to locally credential providers • Medical liaison to all physicians in the community • Link EMS to academic ties within emergency medicine • Linkage of EMS to Public Health initiatives • Oversight of any medical aspect of each service subsystem • ICS: physician @ MCIs, drills, mass gatherings, multiple alarms
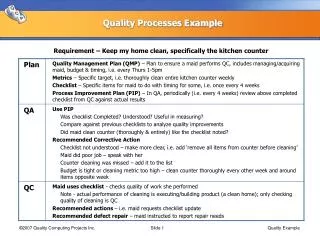
The Medical Review Process • Physicians help adopt a QA Process • Maryland mandates MRC in each county • The physician may have various roles in such a process • Committee may report to him/her • Doc may sit on a committee, or be staff • Provides a buffer panel to avoid extremes of personal opinion, avoid unfairness
Low and High Profile Case • Key step is appropriate fact finding/investigation • Routine case: Mild shortcoming or bad habit • System or an educational mentoring fix • Most states require absolute protection of public in high profile cases • Consider suspending privileges if serious • Medical duties may still include remediation • MD Title 30 requires submission of plans to fix
Studies To Consider EMS “Treat and Release” programs are risky • 10 studies presented at NAEMSP 2003 • In Maryland, study found 2000 ICD-9 codes were encountered by medics in Baltimore • The best under triage rate for treat & release 10% • So why do we need ALS as a means to decide not to transport?
Prehosp Emerg Care. 1999 Apr-Jun;3(2):140-9. Bissell, Seaman et al. • “Change the scope of practice of paramedics? An EMS/public health policy perspective” • 5259 patients transported by city ambulance • ED records available for 3329 (63%) • Top 51 diagnoses accounted for 53.56% • 82.5% of these involve infections, general patient evaluations, and injuries • Each additional diagnosis accounts for less than one-third of 1% of cases
Author's Comments • “The sheer breadth of diagnoses demonstrated a complexity beyond the grasp of any provider without numerous laboratory, diagnostic, and treatment resources.” • How can an EMS provider at any level identify the benign amongst such a high number of illnesses without more training? (Stone ’05)
Prehosp Emerg Care. 2001 Oct-Dec;5(4):360-5 Study To Consider Can basic life support personnel safely determine that advanced life support is not needed? • Questions whether BLS can always judge the lack of need for ALS • N=69; 52 thought not to need ALS;40 needed ALS; 39 high risk CC’s;16 admitted • One of the most debated issues
Study To Consider N Engl J Med. 2004 Aug 12;351(7):647-56. Stiel et all EMT-D programs impact cardiac arrests as much as the average EMT-P Advanced cardiac life support in out-of-hospital cardiac arrest • “OPALS” Study presented at NAEMSP 2004 • The addition of full ALS no better in cardiac arrest than adding AED to EMT-B • ALS valuable in the deteriorating Priority 1 patient
Sub Optimal Outcomes • BLS waives off ALS • ALS on scene derails BLS plan to transport • ALS downgrades a call inappropriately • ALS wishes to stop resuscitation early on • People rely on only one medic who is the errant one Have a common theme
Common Scenarios • Doctor, can I give this to the EMT’s? • Doc, can I get a “priority 4-stop CPR”? • Can you take this “mild trauma” patient? • Doc, I gave him sugar and he woke up; permission for non-transport? • Can I have an order for CPAP? • “A medic was there and said it was OK!”