Download
1 / 1
10 likes | 146 Views
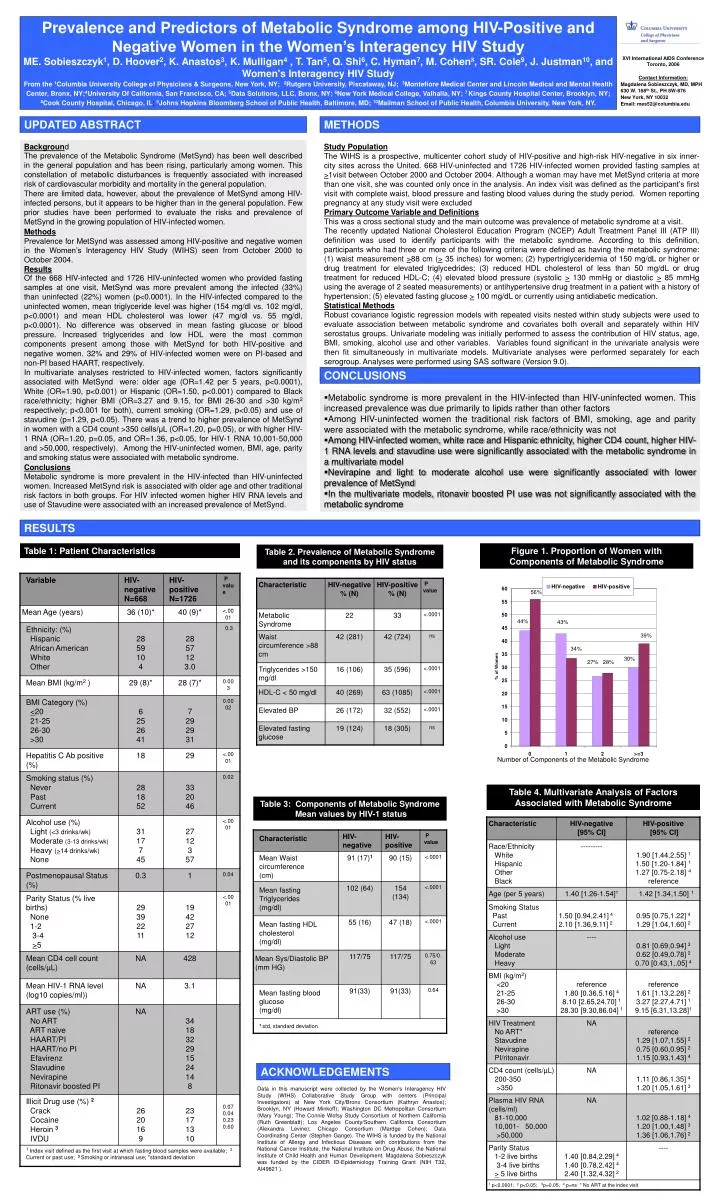
Prevalence and Predictors of Metabolic Syndrome among HIV-Positive and Negative Women in the Women’s Interagency HIV Study

E N D
Prevalence and Predictors of Metabolic Syndrome among HIV-Positive and Negative Women in the Women’s Interagency HIV Study ME. Sobieszczyk1, D. Hoover2, K. Anastos3, K. Mulligan4 , T. Tan5, Q. Shi6, C. Hyman7, M. Cohen8, SR. Cole9, J. Justman10, and Women's Interagency HIV Study From the 1Columbia University College of Physicians & Surgeons, New York, NY; 2Rutgers University, Piscataway, NJ; 3Montefiore Medical Center and Lincoln Medical and Mental Health Center, Bronx, NY;4University Of California, San Francisco, CA; 5Data Solutions, LLC, Bronx, NY; 6New York Medical College, Valhalla, NY; 7 Kings County HospitalCenter, Brooklyn, NY;8Cook County Hospital, Chicago, IL; 9Johns Hopkins Bloomberg School of Public Health, Baltimore, MD; 10Mailman School of Public Health,Columbia University, New York, NY. XVI International AIDS Conference Toronto, 2006 Contact Information: Magdalena Sobieszczyk, MD, MPH 630 W. 168th St., PH 8W-876 New York, NY 10032 Email: mes52@columbia.edu UPDATED ABSTRACT METHODS Background The prevalence of the Metabolic Syndrome (MetSynd) has been well described in the general population and has been rising, particularly among women. This constellation of metabolic disturbances is frequently associated with increased risk of cardiovascular morbidity and mortality in the general population. There are limited data, however, about the prevalence of MetSynd among HIV-infected persons, but it appears to be higher than in the general population. Few prior studies have been performed to evaluate the risks and prevalence of MetSynd in the growing population of HIV-infected women. Methods Prevalence for MetSynd was assessed among HIV-positive and negative women in the Women’s Interagency HIV Study (WIHS) seen from October 2000 to October 2004. Results Of the 668 HIV-infected and 1726 HIV-uninfected women who provided fasting samples at one visit, MetSynd was more prevalent among the infected (33%) than uninfected (22%) women (p<0.0001). In the HIV-infected compared to the uninfected women,mean triglyceride level was higher (154 mg/dl vs. 102 mg/dl, p<0.0001) and mean HDL cholesterol was lower (47 mg/dl vs. 55 mg/dl, p<0.0001). No difference was observed in mean fasting glucose or blood pressure. Increased triglycerides and low HDL were the most common components present among those with MetSynd for both HIV-positive and negative women. 32% and 29% of HIV-infected women were on PI-based and non-PI based HAART, respectively. In multivariate analyses restricted to HIV-infected women, factors significantly associated with MetSyndwere: older age (OR=1.42 per 5 years, p<0.0001), White (OR=1.90, p<0.001) or Hispanic (OR=1.50, p<0.001) compared to Black race/ethnicity; higher BMI (OR=3.27 and 9.15, for BMI 26-30 and >30 kg/m2 respectively; p<0.001 for both), current smoking (OR=1.29, p<0.05) and use of stavudine (p=1.29, p<0.05). There was a trend to higher prevalence of MetSynd in women with a CD4 count >350 cells/μL (OR=1.20, p=0.05), or with higher HIV-1 RNA (OR=1.20, p=0.05, and OR=1.36, p<0.05, for HIV-1 RNA 10,001-50,000 and >50,000, respectively). Among the HIV-uninfected women, BMI, age, parity and smoking status were associated with metabolic syndrome. Conclusions Metabolic syndrome is more prevalent in the HIV-infected than HIV-uninfected women. Increased MetSynd risk is associated with older age and other traditional risk factors in both groups. For HIV infected women higher HIV RNA levels and use of Stavudine were associated with an increased prevalence of MetSynd. Study Population The WIHS is a prospective, multicenter cohort study of HIV-positive and high-risk HIV-negative in six inner-city sites across the United. 668 HIV-uninfected and 1726 HIV-infected women provided fasting samples at >1visit between October 2000 and October 2004. Although a woman may have met MetSynd criteria at more than one visit, she was counted only once in the analysis. An index visit was defined as the participant’s first visit with complete waist, blood pressure and fasting blood values during the study period. Women reporting pregnancy at any study visit were excluded Primary Outcome Variable and Definitions This was a cross sectional study and the main outcome was prevalence of metabolic syndrome at a visit. The recently updated National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) definition was used to identify participants with the metabolic syndrome. According to this definition, participants who had three or more of the following criteria were defined as having the metabolic syndrome: (1) waist measurement >88 cm (> 35 inches) for women; (2) hypertriglyceridemia of 150 mg/dL or higher or drug treatment for elevated triglycedrides; (3) reduced HDL cholesterol of less than 50 mg/dL or drug treatment for reduced HDL-C; (4) elevated blood pressure (systolic > 130 mmHg or diastolic > 85 mmHg using the average of 2 seated measurements) or antihypertensive drug treatment in a patient with a history of hypertension; (5) elevated fasting glucose > 100 mg/dL or currently using antidiabetic medication. Statistical Methods Robust covariance logistic regression models with repeated visits nested within study subjects were used to evaluate association between metabolic syndrome and covariates both overall and separately within HIV serostatus groups. Univariate modeling was initially performed to assess the contribution of HIV status, age, BMI, smoking, alcohol use and other variables. Variables found significant in the univariate analysis were then fit simultaneously in multivariate models. Multivariate analyses were performed separately for each serogroup. Analyses were performed using SAS software (Version 9.0). CONCLUSIONS • Metabolic syndrome is more prevalent in the HIV-infected than HIV-uninfected women. This increased prevalence was due primarily to lipids rather than other factors • Among HIV-uninfected women the traditional risk factors of BMI, smoking, age and parity were associated with the metabolic syndrome, while race/ethnicity was not • Among HIV-infected women, white race and Hispanic ethnicity, higher CD4 count, higher HIV-1 RNA levels and stavudine use were significantly associated with the metabolic syndrome in a multivariate model • Nevirapine and light to moderate alcohol use were significantly associated with lower prevalence of MetSynd • In the multivariate models, ritonavir boosted PI use was not significantly associated with the metabolic syndrome RESULTS Table 1: Patient Characteristics Figure 1. Proportion of Women with Components of Metabolic Syndrome Table 2. Prevalence of Metabolic Syndrome and its components by HIV status 56% 44% 43% 39% 34% 30% 27% 28% Number of Components of the Metabolic Syndrome Table 4. Multivariate Analysis of Factors Associated with Metabolic Syndrome Table 3: Components of Metabolic Syndrome Mean values by HIV-1 status ACKNOWLEDGEMENTS Data in this manuscript were collected by the Women's Interagency HIV Study (WIHS) Collaborative Study Group with centers (Principal Investigators) at New York City/Bronx Consortium (Kathryn Anastos); Brooklyn, NY (Howard Minkoff); Washington DC Metropolitan Consortium (Mary Young); The Connie Wofsy Study Consortium of Northern California (Ruth Greenblatt); Los Angeles County/Southern California Consortium (Alexandra Levine); Chicago Consortium (Mardge Cohen); Data Coordinating Center (Stephen Gange). The WIHS is funded by the National Institute of Allergy and Infectious Diseases with contributions from the National Cancer Institute, the National Institute on Drug Abuse, the National Institute of Child Health and Human Development. Magdalena Sobieszczyk was funded by the CIDER ID-Epidemiology Training Grant (NIH T32, AI49821).